
Histological evaluation of the effectiveness of increased apical enlargement for cleaning the apical third of curved canals
Abstract
Objective: To evaluate the influence of apical size on cleaning of the apical third of curved canals prepared with rotary instruments.
Methodology: Forty-four mesiobuccal canals of maxillary molars teeth were instrumented to different apical sizes (30, 0.02; 35, 0.02; 40, 0.02; 45, 0.02) using a crown-down technique. After canal preparation, the apical thirds of the roots were submitted to histological processing and examination. The specimens were analysed at 40x magnification and the images were submitted to morphometric analysis with an integration grid to evaluate the percentage of debris and uninstrumented root canal walls. The action of the instruments on the root canal walls was assessed based on the surface regularity, abrupt change on the continuity of root canal walls, and partial or total pre-dentine removal. The results were statistically compared using one-way anova with post hoc Tukey test. Pearson’s correlation was performed to identify potential correlations between values.
Results: The percentage of uninstrumented root canal dentine was higher when apical enlargement was performed with instruments 30, 0.02 taper (55.64 ± 4.62%) and 35, 0.02 taper (49.03 ± 5.70%) than with instruments 40, 0.02 taper (38.08 ± 10.44%) and 45, 0.02 taper (32.65 ± 8.51%) (P < 0.05). More debris were observed when apical enlargement was performed with instruments 30, 0.02 taper (34.62 ± 9.49%) and 35, 0.02 taper (25.33 ± 7.37%) (P < 0.05). There was a significant correlation between the amount of remaining debris and the perimeter of uninstrumented root canal dentine (r = 0.9130, P < 0.001).
Conclusion: No apical enlargement size allowed the root canal walls to be prepared completely. Apical third cleanliness could be predicted by instrument diameter.
Introduction
The major goal of root canal treatment is to remove microorganisms from the root canal system to prevent or heal apical periodontitis (Baugh & Wallace 2005, Haapasalo et al. 2005). This is currently achieved by mechanically shaping and chemically cleaning the root canal system (Peters 2004, Paqué et al. 2009). Although many advances have been made in endodontics in the last decades, canal preparation is still adversely influenced by the highly variable root canal anatomy (Peters 2004, Falk & Sedgley 2005).
According to Tan & Messer (2002a,b), effective canal debridement relies on accurate determination of the working length (WL) than adequate apical canal enlargement, as it can overcome the potential limits of irrigation in the apical area, optimizing root canal disinfection (Parris et al. 1994, Yared & Dagher 1994, Siqueira et al. 1997, Albrecht et al. 2004). Conversely, it was demonstrated that root canal debridement improved with progressively larger instrumentation, although no instrumentation technique ensured the elimination of all debris and bacteria (Yared & Dagher 1994, Coldero et al. 2002, Rollison et al. 2002, Usman et al. 2004, Haapasalo et al. 2005).
In the majority of the studies, postoperative root canal cleanliness has been evaluated in relation to debris and smear layer. Overall, no completely cleaned root canals could be found regardless of the instrumentation technique investigated (Hülsmann et al. 2005). Whereas most of the debris was removed, different degrees of smear layer were found in all root canals (Lumley et al. 1993, Parris et al. 1994, Siqueira et al. 1997, Peters & Barbakow 2000, Walters et al. 2002, Weiger et al. 2002, Albrecht et al. 2004, Usman et al. 2004, Falk & Sedgley 2005, Gutarts et al. 2005, Khademi et al. 2006, Sasaki et al. 2006, Grande et al. 2007, Zmener et al. 2009). Debris may be defined as dentine chips, tissue remnants and particles loosely attached to the root canal wall (Hülsmann et al. 2005), whilst the smear layer is a surface film of debris retained on dentine or other surfaces after instrumentation with either rotary instruments or endodontic files (AAE 2003).
There are varying philosophies with regard to the optimal size and shape of root canal preparation; however, there still remains some controversy as to whether apical enlargement is necessary (Yared & Dagher 1994, Coldero et al. 2002, Rollison et al. 2002, Tan & Messer 2002b, Albrecht et al. 2004, Falk & Sedgley 2005, Bartha et al. 2006). A common recommendation is to enlarge the root canal to at least three sizes beyond the initial file to bind (Weine 1972). This recommendation is a matter of debate as the determination of first file that binds does not correlate with the true apical dimension (Wu et al. 2002, Pécora et al. 2005, Vanni et al. 2005), and it is unclear whether enlarging by 3 sizes will adequately remove dentine circumferentially from the root canal walls (Tan & Messer 2002a,b, Usman et al. 2004, Baugh & Wallace 2005, Weiger et al. 2006). On the other hand, minimal apical enlargement has been suggested to conserve tooth structure and limit extrusion of filling materials (Buchanan 1998).
It has been demonstrated that cleaning of the root canal is not always easily accomplished, especially during the preparation of narrow and curved canals (Parris et al. 1994, Peters 2004, Haapasalo et al. 2005, Hülsmann et al. 2005, Zmener et al. 2009). Besides, to secure effective apical cleaning, the instruments should be in contact with every part of the canal wall (Peters 2004, Haapasalo et al. 2005, Hülsmann et al. 2005, Paqué et al. 2009). To deal with this complex problem, several instrumentation techniques and modified instrument designs have been proposed and popularized (Peters 2004, Hülsmann et al. 2005).
In modern endodontic practice, a move has been seen towards the use of engine-driven rotary instrumentation with nickel–titanium (NiTi) instruments (Peters & Barbakow 2000, Barbizam et al. 2002, Coldero et al. 2002, Rollison et al. 2002, Tan & Messer 2002a,b, Weiger et al. 2002, 2006, Peters 2004, Usman et al. 2004, Gutarts et al. 2005, Sasaki et al. 2006, Paqué et al. 2009, Pasternak-Junior et al. 2009, Zmener et al. 2009), because they promote significantly less canal transportation than conventional files, providing more centred and tapered preparations (Peters 2004, Hülsmann et al. 2005, Versiani et al. 2008, Pasternak-Junior et al. 2009). However, these findings underline the limited efficiency of endodontic instruments in cleaning the apical part of the root canal and the importance of additional irrigation as crucial for sufficient disinfection of the canal system (Hülsmann et al. 2005).
The purpose of this study was to evaluate the influence of apical enlargement size on the cleaning of the apical third of mesiobuccal root canals of maxillary molars prepared with Hero 642 rotary system, through histological evaluation.
Material and methods
After ethics committee approval (Protocol #084/05), forty-four mesiobuccal canals of freshly extracted human maxillary molar teeth with fully formed apices displaying patent and separate root canals, with an angle of curvature raging from 20 to 40° and a radius of curvature less than 10 mm, were selected and stored in distilled water until use. The occlusal one-half of each crown was removed with a high-speed handpiece and tapered diamond bur to create a flat surface for easier access to the pulp chamber and to facilitate length measurement of the canal.
After conventional access preparations, the cervical and middle thirds were enlarged with NiTi rotary instruments sizes 25, 0.12 taper, 25, 0.10 taper and 25, 0.08 taper (Micro-Mega, Besançon, France) used serially in a crown-down technique towards the apex. Flaring was followed by irrigation with distilled water delivered in a syringe with a 30-gauge NaviTip™ needle (Ultradent Products Inc., South Jordan, UT, USA). Apical patency was determined by inserting a size 08 K-file into the root canal until the tip of the file was visible at the apical foramen; the WL was set 1.0 mm short of this measurement. Then, stainless steel K-files (Dentsply Maillefer, Ballaigues, Switzerland), with progressively larger tip diameter, were inserted passively to the WL with a light ‘watch-winding’ action for measuring apical canal diameter. Care was taken to avoid any force during sizing. Only canals in which the final apical gauging allowed for a size 20 hand file to be placed to the WL were included.
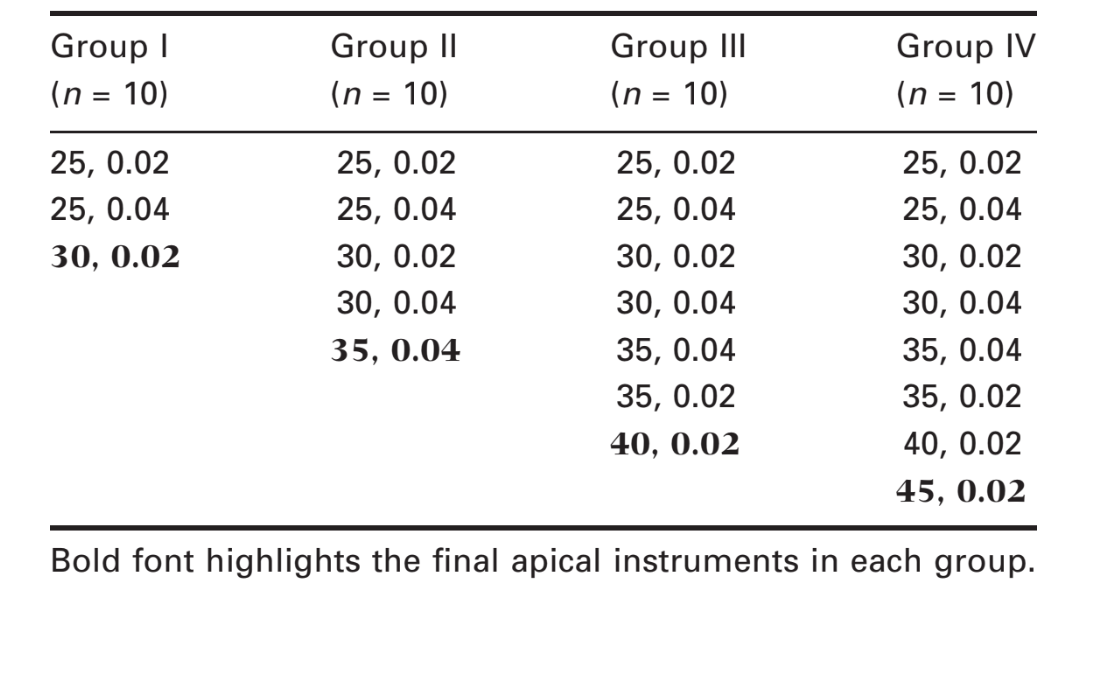
The canals were randomly assigned into 4 experimental groups (n = 10) according to the apical enlargement (Table 1) and stratified in such a manner that the averages of the root canal length and curvature were as close to each other as possible. The negative control group included two uninstrumented and unirrigated root canals. In the positive control group, two canals had no mechanical preparation; instead, irrigation with distilled water was performed so that the specimens were exposed to the same volume of irrigant for the same length of time. To avoid instrument fracture, five canals were instrumented with one set of NiTi rotary instruments (Hero 642; Micro-Mega) at the WL, driven by a controlled high torque motor (Endo Plus; Driller, São Paulo, SP, Brazil) set to 300 rpm. During all procedures, the teeth were wrapped in wet gauze and the canals were flushed with 2 mL of distilled water between each instrument, delivered in a syringe with a 30-gauge needle placed 1 mm short of the WL. In addition, to achieve a certain degree of uniformity and reduce interoperator variables, all experimental procedures were conducted by the same operator.
After root canal preparation, all specimens were immersed in 10% buffered formalin for 48 h. The teeth were then washed in running water for 1 h and decalcified in 10% trichloroacetic acid for 15 days. The decalcified roots were cut perpendicularly to their long axis with a scalpel at 5 mm from anatomical apex and embedded in paraffin. Care was taking to avoid contamination during the sectioning process. Serial sections (10 semi-serial sections of each specimen) with 6-lm thickness were cut, stained with haematoxylin and eosin (H&E), and examined under an optical microscope (Eclipse E 600; Nikon, Shinagawaku, Tokyo, Japan), coupled to a computer, at 40x magnification. Before viewing the sections, any identification on the slide was masked and the slides randomized, allowing blinded evaluation that was undertaken by two trained observers.
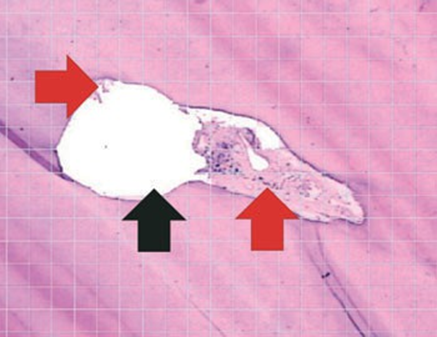
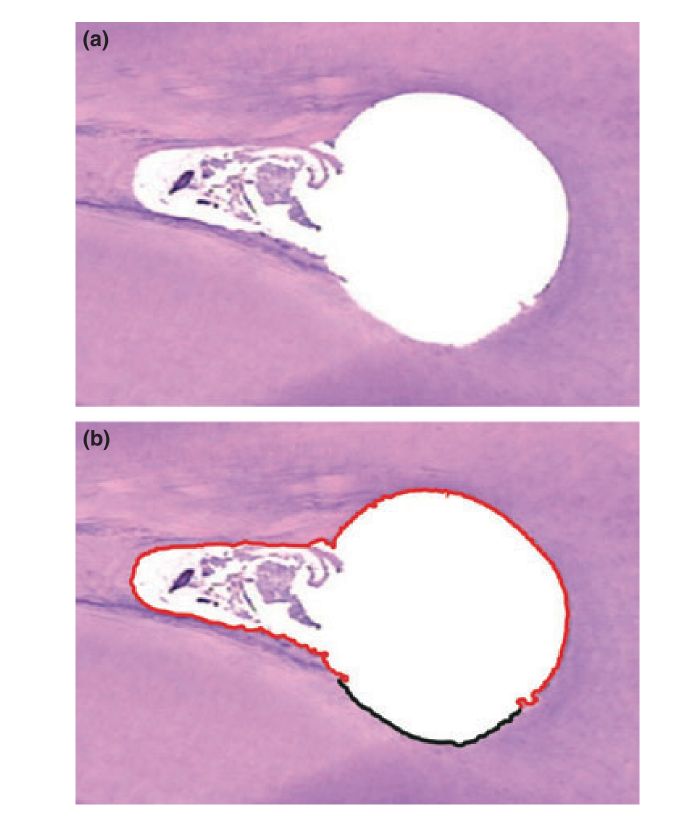
The images were recorded as a tagged image file format (Adobe Premiere 5.1; Adobe Systems Incorporated, San Jose, USA) and evaluated for the percentage of debris and uninstrumented root canal walls. The percentage of debris was calculated by placing an integration grid (Corel Photo Paint 12; Corel Corp., Ottawa, ON, Canada) over the cross-section images to allow counting the points in the root canal that coincided with either clean areas or areas containing debris (Figure 1). The percentage of uninstrumented root canal walls was determined by calculating the length of the canal outline that was not touched by the instruments in relation to the total length of the canal outline, using Scion Image software (Scion Corporation, Frederick, MD, USA) (Figure 2). The action of the instruments on the root canal walls was assessed based on the following criteria: surface regularity, abrupt change on the continuity of root canal wall, and partial or total pre-dentine removal. The prepared root canal outline was traced in a different colour to differentiate it from the uninstrumented canal.
The mean percentages of remaining debris and uninstrumented root canal perimeter at the apical third, considering different apical enlargement, were statistically compared using one-way anova with post hoc Tukey test. Pearson’s correlation was performed to determine correlations between the analysed values.
Results
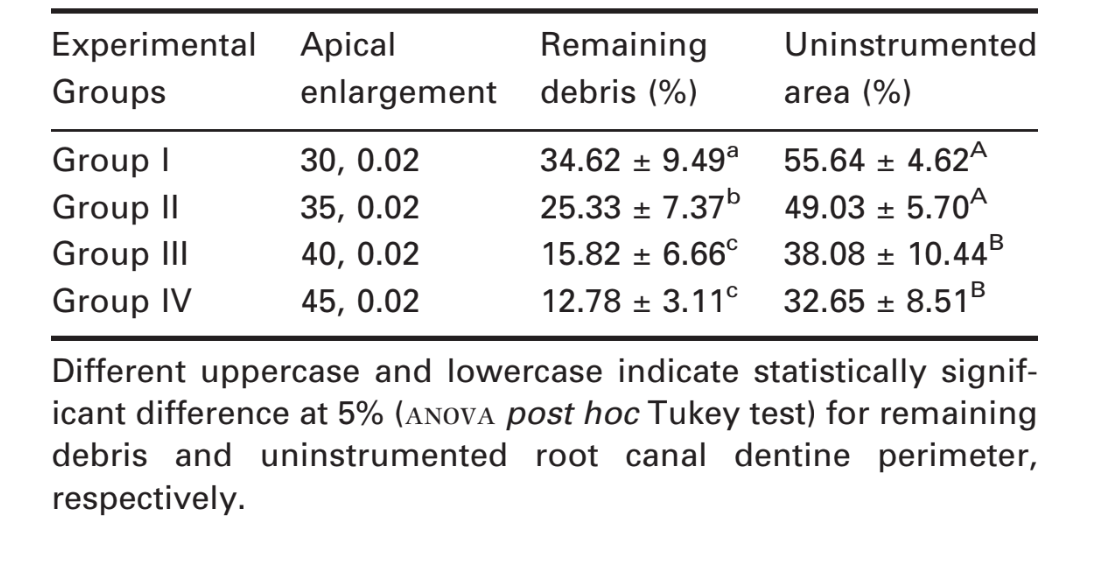
The results of the analysis of the root canal cleanliness are detailed in Table 2. All experimental groups revealed significantly less debris and uninstrumented root canal walls than negative and positive control groups (P < 0.001). The percentage of remaining debris that was observed was not significantly different when apical enlargement was performed with instruments 40, 0.02 taper (15.82 ± 6.66%) and 45, 0.02 taper (12.78 ± 3.11%) (P > 0.05). More debris were observed when apical enlargement was performed with instruments 30, 0.02 taper (34.62 ± 9.49%) and 35, 0.02 taper (25.33 ± 7.37%) (P < 0.05). The percentage of uninstrumented root canal dentine was higher when apical enlargement was performed with instruments 30, 0.02 taper (55.64 ± 4.62%) and 35, 0.02 taper (49.03 ± 5.70%) than with instruments 40, 0.02 taper (38.08 ± 10.44%) and 45, 0.02 taper (32.65 ± 8.51%) (P < 0.05). A highly significant correlation between the amount of remaining debris and the perimeter of uninstrumented root canal dentine was observed (r = 0.9130, P < 0.001).
Discussion
As root canal anatomy of molars is variable and they generally pose clinical problems (Vanni et al. 2005, Bartha et al. 2006, Paqué et al. 2009, Pasternak-Junior et al. 2009), mesiobuccal roots of maxillary molars were used. An attempt was made to balance the experimental groups with respect to tooth type, root canal curvature and the smallest canal diameter gauged at the most apical region because these parameters seem to have an impact on the instrumentation results (Peters et al. 2003, Peters 2004, Hülsmann et al. 2005, Bartha et al. 2006, Versiani et al. 2008).
To determine the appropriate final diameter needed for complete apical enlargement, pre-flaring of the coronal and middle thirds has been recommended prior to determining the initial file that binds (Wu et al. 2002, Baugh & Wallace 2005, Pécora et al. 2005, Vanni et al. 2005). Apical gauging is the measurement of the terminal diameter or shape of a canal after initial crown-down shaping (AAE 2003) and has been advocated for determination of apical preparation size (Tan & Messer 2002b, Baugh & Wallace 2005, Falk & Sedgley 2005, Vanni et al. 2005, Bartha et al. 2006, Weiger et al. 2006). Although there is disagreement amongst endodontic specialists about the ideal apical diameter of the root canal preparation, there is universal agreement that the ideal size varies from tooth to tooth and depends on anatomical, microbiological and mechanical factors (Peters 2004, Baugh & Wallace 2005).
In this study, the root canals were pre-flared and conventional files were used for apical sizing as this procedure reflects clinical conditions under which root canal treatment is performed (Tan & Messer 2002a, Bartha et al. 2006, Weiger et al. 2006). The minimum apical enlargement was based on the evidence that the minimum instrumentation size needed for penetration of irrigant to the apical third of the root canal is a size 30 file (Rollison et al. 2002, Usman et al. 2004, Baugh & Wallace 2005, Falk & Sedgley 2005, Haapasalo et al. 2005, Khademi et al. 2006).
The predictability of the preparation techniques has been influenced by the design and alloy of the instruments; nevertheless, the tactile skills of the operator have been considered more important than the technique in the thoroughness of canal debridement (Peters 2004, Gutarts et al. 2005, Hülsmann et al. 2005). Thus, in this study, root canal preparations were carried out by an endodontist with expertise in rotary techniques.
The majority of studies provide a strong consensus that larger apical preparation size not only allows proper irrigation but also results in a greater reduction in the remaining bacteria and dentinal debris compared with smaller apical preparation sizes (Yared & Dagher 1994, Coldero et al. 2002, Rollison et al. 2002, Falk & Sedgley 2005, Haapasalo et al. 2005). Despite the fact that larger apical preparation sizes produced a greater reduction in dentinal debris in comparison with smaller apical preparation sizes, this study confirmed previous investigations that reported neither technique nor apical enlargement completely cleaned root canal walls (Parris et al. 1994, Wu & Wesselink 1995, Siqueira et al. 1997, Barbizam et al. 2002, Weiger et al. 2002, Usman et al. 2004, Baugh & Wallace 2005, Haapasalo et al. 2005, Sasaki et al. 2006, Zmener et al. 2009).
Parris et al. (1994) reported that the rotation of the final largest file at WL following irrigation and drying of the canal systems effectively removed debris remaining on the walls in the apical third. Siqueira et al. (1997) and Wu & Wesselink (1995) demonstrated that although bacterial reduction occurred during apical enlargement, complete debridement was impossible. Card et al. (2002) demonstrated a significant reduction in remaining bacteria when mesial roots of mandibular molars were instrumented to size 60. Rollison et al. (2002) showed larger file sizes to a size 50 produced a greater reduction in remaining bacteria than those instrumented with a size 35. Tan & Messer (2002a,b) and Usman et al. (2004) concluded that no technique was totally effective in cleaning the apical canal space, but larger instrumentation was beneficial in reducing debris in the apical third of canals. Bartha et al. (2006) concluded that even a wide apical enlargement did not result in complete cutting of canal walls. In addition, several comparative investigations of pre- and postoperative cross-sections of mesiobuccal root canals in curved mandibular molars resulted in 3 to 18 out of 25 specimens with more than 25% of the diameter left unprepared following preparation with different rotary NiTi systems to size 45 (Hülsmann et al. 2001, 2003a,b, Versümer et al. 2002, Paqué et al. 2005, Kahlmeier & Hülsmann 2007).
In the apical region, root canals tend towards a rounder cross-section as the long diameter of oval canals decreases apically (Wu et al. 2000). In most cases, this may allow a wider enlargement with suitable flexible NiTi rotary instruments. Overall, the ability of NiTi instruments to achieve better canal cleanliness scores than hand instrumentation was due primarily to the fact that this instrument could remain centred and hence allow most surfaces of the canal wall to be planed (Tan & Messer 2002b, Peters 2004, Hülsmann et al. 2005, Versiani et al. 2008). Besides, although flexible rotary NiTi instruments allow the preparation of curved root canals to a large diameter, irrigation and the use of an intracanal dressing such as calcium hydroxide may overcome these anatomical complexities (Walters et al. 2002, Peters 2004, Baugh & Wallace 2005, Haapasalo et al. 2005, Bartha et al. 2006).
Many rotary instrumentation techniques tend to produce round preparations (Peters 2004, Hülsmann et al. 2005, Versiani et al. 2008, Pasternak-Junior et al. 2009) leaving areas of the canal wall uninstrumented, especially in oval canals (Lumley et al. 1993, Wu et al. 2000, Weiger et al. 2002). Inevitably, as the canal is not instrumented in these regions the infected inner layer of dentine will remain. Though, from a microbiological point of view there are no valid data on the amount of dentine that should be removed in cases with root canal wall infection to promote apical healing or prevent the formation of an apical lesion (Peters 2004, Usman et al. 2004, Baugh & Wallace 2005, Haapasalo et al. 2005) once necrotic pulp remnants and bacteria may remain even in an adequately gauged canal (Yared & Dagher 1994, Coldero et al. 2002, Rollison et al. 2002, Falk & Sedgley 2005).
This study did not evaluate the cleaning capacity of irrigating solutions. Nonetheless, there is evidence that the flushing action of the irrigant solution may be more important during the cleaning process than the ability of the irrigant solution to dissolve tissue (Peters & Barbakow 2000).
According to some authors, when the apical diameter is measured by a conventionally tapered file, the apical preparation size should be at least 6–8 file sizes larger than the first apical biding file as this first file may not reflect the real apical diameter (Peters & Barbakow 2000, Wu et al. 2002, Usman et al. 2004, Baugh & Wallace 2005, Pécora et al. 2005, Vanni et al. 2005, Bartha et al. 2006, Weiger et al. 2006). Thus, further studies on the combination of apical enlargement with different rotary systems, hand files used in a circumferential manner, ultrasonic irrigation and various irrigant solutions should be performed. This will allow establishing protocols that associate different instruments and chemical irrigant that would result in a more effective root canal cleaning.
Conclusion
Within the limitations of this study, it can be concluded that file sizes to a 40, 0.02 taper and 45, 0.02 taper produced a greater reduction in remaining debris and untouched root canal walls than those instrumented with 30, 0.02 taper and 35, 0.02 taper files at the apical third of mesiobuccal roots of maxillary molars. Nevertheless, no apical enlargement size could prepare root canal walls completely. Pearson’s correlation revealed that apical third cleanliness could be predicted by instrument size.
Authors: V. J. Fornari, Y. T. C. Silva-Sousa, J. R. Vanni, J. D. Pécora, M. A. Versiani, M. D. Sousa-Neto
References:
- AAE (2003) Glossary of endodontics terms, 7th edn. Chicago: American Association of Endodontists.
- Albrecht LJ, Baumgartner JC, Marshall JG (2004) Evaluation of apical debris removal using various sizes and tapers of ProFile GT files. Journal of Endodontics 30, 425–8.
- Barbizam JV, Fariniuk LF, Marchesan MA, Pécora JD, Sousa-Neto MD (2002) Effectiveness of manual and rotary instrumentation techniques for cleaning flattened root canals. Journal of Endodontics 28, 365–6.
- Bartha T, Kalwitzki M, Löst C, Weiger R (2006) Extended apical enlargement with hand files versus rotary NiTi files. Part II. Oral Surgery, Oral Medicine, Oral Patholology, Oral Radiology, and Endodontics 102, 692–7.
- Baugh D, Wallace J (2005) The role of apical instrumentation in root canal treatment: a review of the literature. Journal of Endodontics 31, 333–40.
- Buchanan LS (1998) The standardized-taper root canal preparation, part 1: concepts for variably tapered shaping instruments. Dentistry Today 17, 54–60.
- Card SJ, Sigurdsson A, Ørstavik D, Trope M (2002) The effectiveness of increased apical enlargement in reducing intracanal bacteria. Journal of Endodontics 28, 779–83.
- Coldero LG, McHugh S, MacKenzie D, Saunders WP (2002) Reduction in intracanal bacteria during root canal preparation with and without apical enlargement. International Endodontic Journal 35, 437–46.
- Falk KW, Sedgley CM (2005) The influence of preparation size on the mechanical efficacy of root canal irrigation in vitro. Journal of Endodontics 31, 742–5.
- Grande NM, Plotino G, Butti A, Messina F, Pameijer CH, Somma F (2007) Cross-sectional analysis of root canals prepared with NiTi rotary instruments and stainless steel reciprocating files. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics 103, 120–6.
- Gutarts R, Nusstein J, Reader A, Beck M (2005) In vivo debridement efficacy of ultrasonic irrigation following hand-rotary instrumentation in human mandibular molars. Journal of Endodontics 31, 166–70.
- Haapasalo M, Endal U, Zandi H, Coil JM (2005) Eradication of endodontic infection by instrumentation and irrigation solutions. Endodontic Topics 10, 77–102.
- Hülsmann M, Schade M, Schäfers F (2001) A comparative study of root canal preparation with HERO 642 and Quantec SC rotary Ni–Ti instruments. International Endodontic Journal 34, 538–46.
- Hülsmann M, Herbst U, Schäfers F (2003a) A comparative study of root canal preparation using Lightspeed and Quantec SC rotary Ni–Ti instruments. International Endodontic Journal 36, 748–56.
- Hülsmann M, Gressmann G, Schäfers F (2003b) A comparative study of root canal preparation using FlexMaster andHERO642 rotary Ni–Ti instruments. International Endodontic Journal 36, 3358–66.
- Hülsmann M, Peters OA, Dummer PMH (2005) Mechanical preparation of root canals: shaping goals, techniques and means. Endodontic Topics 10, 30–76.
- Kahlmeier C, Hülsmann M (2007) A comparative study of root canal preparation using GT Rotary and ProFile rotary NiTi instruments. Journal of Endodontics 40, 553–62.
- Khademi A, Yazdizadeh M, Feizianfard M (2006) Determination of the minimum instrumentation size for penetration of irrigants to the apical third of root canal systems. Journal of Endodontics 32, 417–20.
- Lumley PJ, Walmsley AD, Walton RE, Rippin JW (1993) Cleaning of oval canals using ultrasonic or sonic instrumentation. Journal of Endodontics 19, 453–7.
- Paqué F, Musch U, Hülsmann M (2005) Comparison of root canal preparation using RaCe and ProTaper rotary Ni–Ti instruments. International Endodontic Journal 38, 8–16.
- Paqué F, Ganahl D, Peters OA (2009) Effects of root canal preparation on apical geometry assessed by micro-computed tomography. Journal of Endodontics 35, 1056–9.
- Parris J, Wilcox L, Walton R (1994) Effectiveness of apical clearing: histological and radiographical evaluation. Journal of Endodontics 20, 219–24.
- Pasternak-Junior B, Sousa-Neto MD, Silva RG (2009) Canal transportation and centring ability of RaCe rotary instruments. International Endodontic Journal 42, 499–506.
- Pécora JD, Capelli A, Guerisoli DM, Spanó JC, Estrela C (2005) Influence of cervical preflaring on apical file size determination. International Endodontic Journal 38, 430–5.
- Peters OA (2004) Current challenges and concepts in the preparation of root canal systems: a review. Journal of Endodontics 30, 559–67.
- Peters OA, Barbakow F (2000) Effects of irrigation on debris and smear layer on canal walls prepared by two rotary techniques: a scanning electron microscopic study. Journal of Endodontics 26, 6–10.
- Peters OA, Peters CI, Schönenberger K, Barbakow F (2003) ProTaper rotary root canal preparation: effects of canal anatomy on final shape analysed by micro CT. International Endodontic Journal 36, 86–92.
- Rollison S, Barnett F, Stevens RH (2002) Efficacy of bacterial removal from instrumented root canals in vitro related to instrumentation technique and size. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics 94, 366–71.
- Sasaki EW, Versiani MA, Perez DE, Sousa-Neto MD, Silva-Sousa YT, Silva RG (2006) Ex vivo analysis of the debris remaining in flattened root canals of vital and nonvital teeth after biomechanical preparation with Ni–Ti rotary instruments. Brazilian Dental Journal 17, 233–6.
- Siqueira JF Jr, Araujo MC, Garcia PF, Fraga RC, Dantas CJ (1997) Histological evaluation of the effectiveness of five instrumentation techniques for cleaning the apical third of root canals. Journal of Endodontics 23, 499–502.
- Tan BT, Messer HH (2002a) The effect of instrument type and preflaring on apical file size determination. International Endodontic Journal 35, 752–8.
- Tan BT, Messer HH (2002b) The quality of apical canal preparation using hand and rotary instruments with specific criteria for enlargement based on initial apical file size. Journal of Endodontics 28, 658–64.
- Usman N, Baumgartner JC, Marshall JG (2004) Influence of instrument size on root canal debridement. Journal of Endodontics 30, 110–2.
- Vanni JR, Santos R, Limongi O, Guerisoli DM, Capelli A, Pécora JD (2005) Influence of cervical preflaring on determination of apical file size in maxillary molars: SEM analysis. Brazilian Dental Journal 16, 181–6.
- Versiani MA, Pascon EA, de Sousa CJ, Borges MA, Sousa- Neto MD (2008) Influence of shaft design on the shaping ability of 3 nickel–titanium rotary systems by means of spiral computerized tomography. Oral Surgery, Oral Medicine, Oral Patholology, Oral Radiology, and Endodontics 105, 807–13.
- Versümer J, Hülsmann M, Schäfers F (2002) A comparative study of root canal preparation using ProFile .04 and Lightspeed rotary NiTi instruments. International Endodontic Journal 35, 37–46.
- Walters MJ, Baumgartner JC, Marshall JG (2002) Efficacy of irrigation with rotary instrumentation. Journal of Endodontics 28, 837–9.
- Weiger R, ElAyouti A, Löst C (2002) Efficiency of hand and rotary instruments in shaping oval root canals. Journal of Endodontics 28, 580–3.
- Weiger R, Bartha T, Kalwitzki M, Löst C (2006) A clinical method to determine the optimal apical preparation size. Part I. Oral Surgery, Oral Medicine, Oral Patholology, Oral Radiology, and Endodontics 102, 686–91.
- Weine F (1972) Endodontic therapy. St. Louis: Mosby.
- Wu MK, Wesselink PR (1995) Efficacy of three techniques in cleaning the apical portion of curved root canals. Oral Surgery, Oral Medicine, Oral Patholology, Oral Radiology, and Endodontics 79, 492–6.
- Wu MK, R’Oris A, Barkis D, Wesselink PR (2000) Prevalence and extent of long oval canals in the apical third. Oral Surgery, Oral Medicine, Oral Patholology, Oral Radiology, and Endodontics 89, 739–43.
- Wu MK, Barkis D, Roris A, Wesselink PR (2002) Does the first file to bind correspond to the diameter of the canal in the apical region? International Endodontic Journal 35, 264–7.
- Yared GM, Dagher FE (1994) Influence of apical enlargement on bacterial infection during treatment of apical periodontitis. Journal of Endodontics 20, 535–7.
- Zmener O, Pameijer CH, Serrano SA, Palo RM, Iglesias EF (2009) Efficacy of the NaviTip FX irrigation needle in removing post instrumentation canal smear layer and debris in curved root canals. Journal of Endodontics 35, 1270–3.