The Radix Entomolaris and Paramolaris: A Micro–Computed Tomographic Study of 3-rooted Mandibular First Molars
Abstract
Introduction: The morphology of the supernumerary third root (radix) in mandibular first molars was examined by micro–computed tomography (mCT) scanning.
Methods: Nineteen permanent mandibular first molars with radix were scanned in a mCT device to evaluate their morphology with respect to root length, root curvature direction, location of radix, apical foramen, accessory canals and apical deltas, and distance between canal orifices as well as 2- and 3-dimensional parameters of the canals (number, area, roundness, major/minor diameter, volume, surface area, and structure model index). Quantitative data were analyzed by 1-way analysis of variance and the Tukey test (α = 0.05).
Results: The mean length of the mesial, distal, and radix roots was 20.36 ± 1.73 mm, 20.0 ± 1.83 mm, and 18.09 ± 1.68 mm, respectively. The radix was located distolingually (n = 16), mesiolingually (n = 1), and distobuccally (n = 2). In a proximal view, most radix roots had a severe curvature with buccal orientation and a buccally displaced apical foramen. The spatial configuration of the canal orifices on the pulp chamber floor was mostly in a trapezoidal shape. The radix root canal orifice was usually covered by a dentinal projection. The radix differed significantly from the mesial and distal roots for all evaluated 3-dimensional parameters (P < .05). The radix canal had a more circular shape in the apical third, and the mean size of the minor diameter 1 mm short of the foramen was 0.25 ± 0.10 mm.
Conclusions: The radix root is an important and challenging anatomic variation of mandibular first molars, which usually has a severe curvature with a predominantly distolingual location, and a narrow root canal with difficult access. (J Endod 2014;■:1–6)
The main goal of endodontic therapy is to obtain 3-dimensional (3D) obturation of the root canal system (RCS) after a sequence of cleaning, shaping, and filling procedures. However, variation in root and RCS anatomy may represent an additional difficulty to the final outcome. Endodontic failure may be associated with the persistence of infection because of a missed canal or inefficient elimination of microorganisms and necrotic pulp remnants during chemomechanical instrumentation. Thorough knowledge of the root and RCS anatomy and their possible variations is mandatory to minimize errors and achieve endodontic success.
Mandibular first molars usually have 2 roots, 1 mesial and 1 distal, and 3 canals, but variations in the number of roots and RCS anatomy are not uncommon. Carabelli was the first to mention the presence of a supernumerary third root as a frequent variation in this tooth group, located either lingually (radix entomolaris) or buccally (radix paramolaris). Three-rooted mandibular first molars deserve special attention during endodontic treatment because the additional root is usually smaller than the mesial and distal roots, can be either separate or partially fused with the other roots, and has a severe curvature in most cases. The occurrence of a third root in the mandibular first molar is associated with certain ethnic groups. The literature reports an incidence of less than 5% in white, African, and Eurasian populations, whereas in populations with Mongoloid traits, such as Chinese, Eskimo, and American Indians, this anatomic variation occurs with a 5%–40% frequency.
Micro–computed tomography (mCT) imaging allows for accurate quantitative and qualitative 3D data acquisition and has emerged as a powerful tool for assessing RCS anatomy in experimental endodontic studies. A 3-part study in a Chinese population used mCT imaging to examine the root canal morphology of permanent 3-rooted mandibular molars with respect to pulp floor and RCS, root curvature, and odontometry, but none of these 3 separate works performed comprehensive quantitative 2-dimensional (2D) and 3D analyses of canal morphology by assessing several morphometric data in the same sample of teeth. In fact, the literature lacks detailed descriptions of the anatomic and morphologic variations of 3-rooted mandibular molars using highly accurate tomographic techniques. Although presently such analyses are not practical to be performed in clinical settings in routine dental practice, laboratory studies using high-quality 3D imaging methods, such as mCT imaging, provide valuable information on root and canal morphology that could increase the safety and efficiency of root canal preparation procedures, especially in teeth with peculiar anatomy, and even support the implementation of new treatment protocols. In the present study, high-resolution mCT imaging was used to examine the internal and external morphology of the supernumerary third root (radix) in mandibular first molars.
Materials and Methods
Nineteen human permanent 3-rooted mandibular first molars were selected from a pool of extracted teeth belonging to our endodontics laboratory collection and were stored in individual plastic vials containing 0.1% thymol solution. The sex, ethnicity, and age of tooth donors were unknown. After washing in running water for 24 hours, the length of the roots was measured from the apex to the cementoenamel junction with a digital caliper, and the location of the additional root was recorded. Then, each tooth was dried, scanned in a mCT scanner (SkyScan 1174v2; Bruker-microCT, Kontich, Belgium) at an isotropic resolution of 22.9 mm, and reconstructed with dedicated software (NRecon v.1.6.3; Bruker-microCT), providing axial cross-sections of the inner structure of the samples.
DataViewer v.1.4.4 software (Bruker-microCT) was used to evaluate the presence and location of accessory canals and apical delta. CTVox v.2.2 and CTVol v.2.4 software (Bruker-microCT) was used for the visualization of 3D models and qualitative evaluation of the root canal configuration, the direction of root curvature from the proximal and buccal views, and apical foramen location. CTAn v.2.2.1 software (Bruker-microCT) was used to measure the distance between the canal orifices on the pulp chamber floor and for 3D analysis of the root canal from the apex to the cementoenamel junction (volume, surface area, and structure model index) and 2D analysis of the root canals at 1, 2, and 3 mm from the apical foramen (number, area, roundness, major diameter, and minor diameter). Because the mesial root can present with either a single canal or 2 canals with different isthmuses, a classification proposed by Weller et al was used for better understanding the dispersion of the 2D results; a complete isthmus had a continuous opening between the 2 main root canals, whereas a partial isthmus was defined as a narrow projection of 1 root canal opening toward the second in the same root section but without merging.
Structure model index (SMI) involves a measurement of surface convexity in a 3D structure. SMI is derived as 6.([S’.V]/S2), where S is the object surface area before dilation and S’ is the change in surface area caused by dilation. V is the initial undilated object volume. An ideal plate, cylinder, and sphere have SMI values of 0, 3, and 4, respectively. The cross-sectional appearance, round or more ribbon shaped, was expressed as roundness. Roundness of a discreet 2D object is defined as 4.A/(π.(dmax)2), where A is the area and dmax is the major diameter. The value of roundness ranges from 0–1, with 1 signifying a circle.
Data from the distance between canal orifices and 2D and 3D parameters were presented as means and standard deviations and statistically analyzed by 1-way analysis of variance and the post hoc Tukey test with a significance level of 5% using SPSS v17.0 for Windows (SPSS Inc, Chicago, IL).
Results
The mean length of the mesial, distal, and radix roots was 10.03 ± 1.32 mm, 9.97 ± 1.84 mm, and 7.65 ± 1.55 mm, respectively. The radix was located distolingually (n = 16), mesiolingually (n = 1), and distobuccally (n = 2).
Regarding the internal anatomy, most accessory canals were found in the apical third. Comparing the thirds, accessory canals were found in the apical third in 11 mesial, 11 distal, and 5 radix roots. In the middle third, accessory canals were found in 2 mesial roots and 1 radix root. No accessory canal was found in the coronal third in any of the roots. Apical delta was observed in the 3 root canals of only 1 specimen (Fig. 1: 5D). 3D model analysis revealed that the RCS of these teeth had different morphologies including 4 or 3 independent canals (Fig. 1: 1D and 2D), isthmuses, and apical deltas (Fig. 1: 3D), middle mesial canal in the mesial root (Fig. 1: 4D), and 2 middle mesial canals joined at the apical third (Fig. 1: 5D).
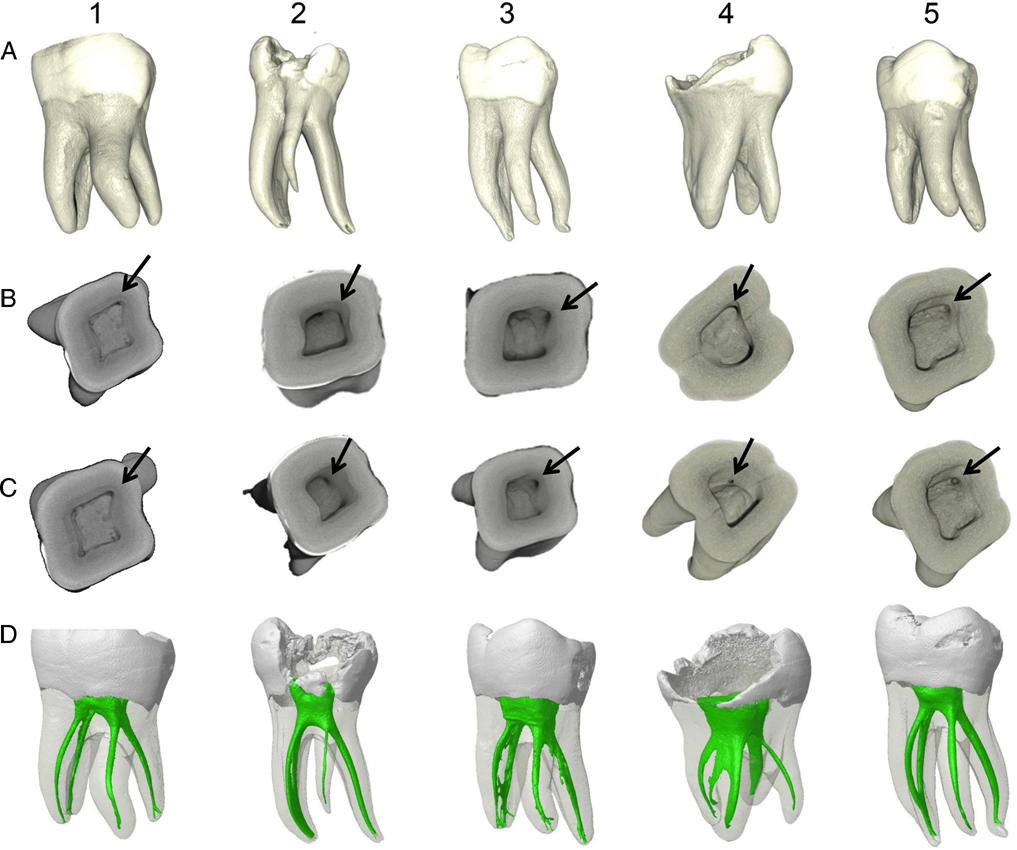
radix. (B and C) coronal view of the pulp chamber showing the position of the radix orifice (arrows) and grooves on the pulp chamber floor. (D) 3D models
showing the internal anatomy of the specimens. Specimen 4 had a middle mesial canal in the mesial root, whereas apical delta could be observed in all canals of specimen 3.
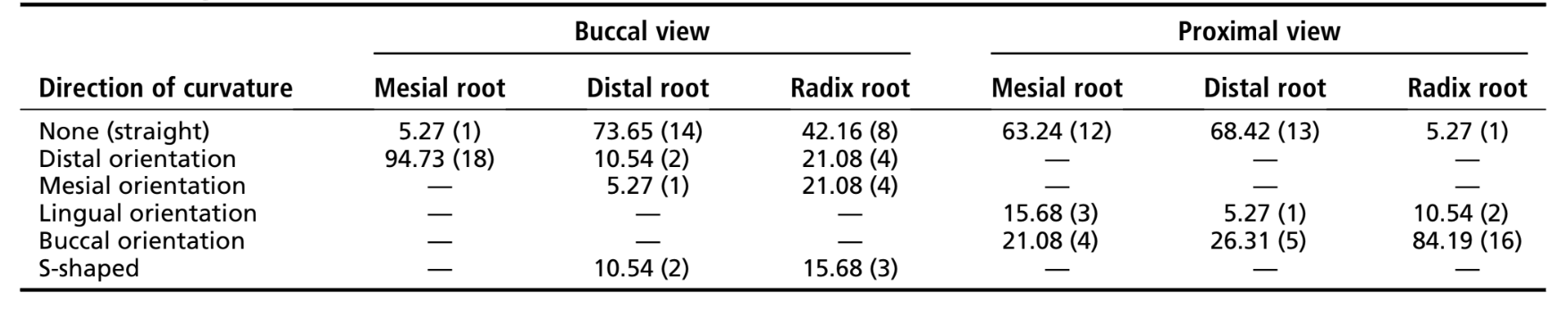
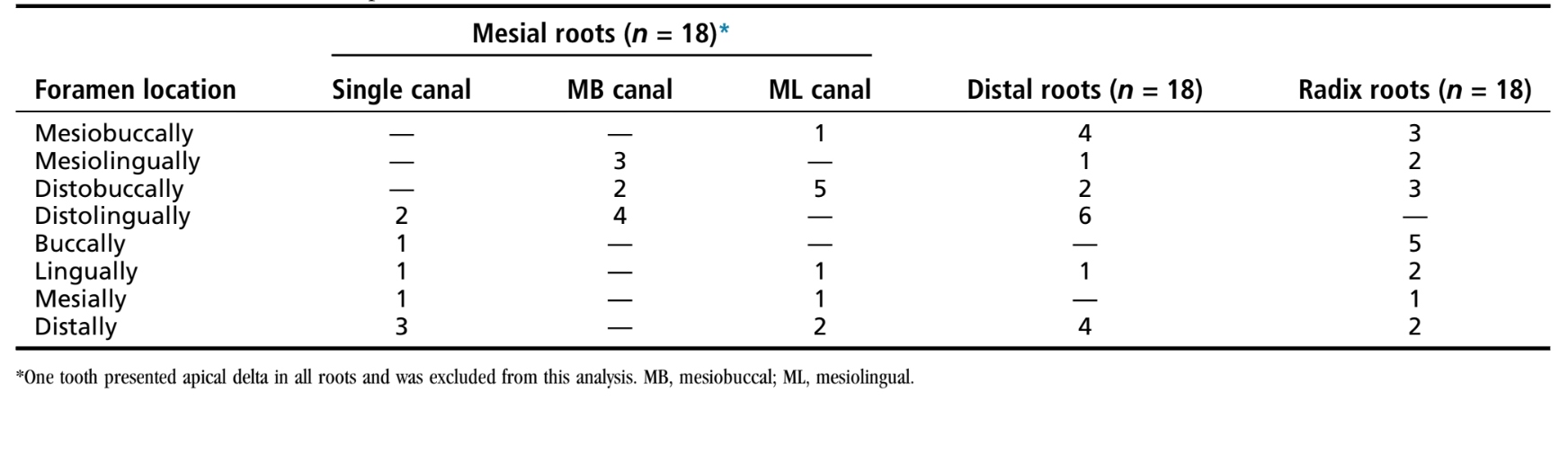
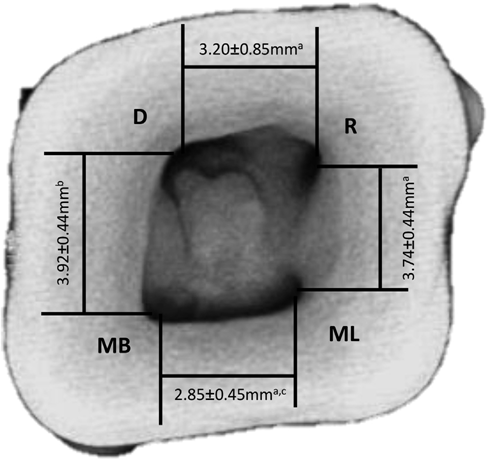
Tables 1 and 2 show the percentage distribution of root curvature direction and apical foramen location, respectively. A proximal view revealed that in most cases the radix had a curvature with buccal orientation (n = 16, 84.19%). The apical foramina also had a tendency to be displaced buccally, mesiobuccally, and distobuccally. This characteristic was also observed in the qualitative analysis of the 3D models, which showed that most radix roots presented a moderate to severe curvature with the apical foramen accompanying the curve (Fig. 2). Therefore, the radix canal orifice is usually covered by a dentin projection of the pulp chamber walls, which makes it difficult to locate during the access surgery (Fig. 1, lines B and C). A trapezoidal spatial configuration of the canal orifices on the pulp chamber floor was mostly observed (Fig. 3).
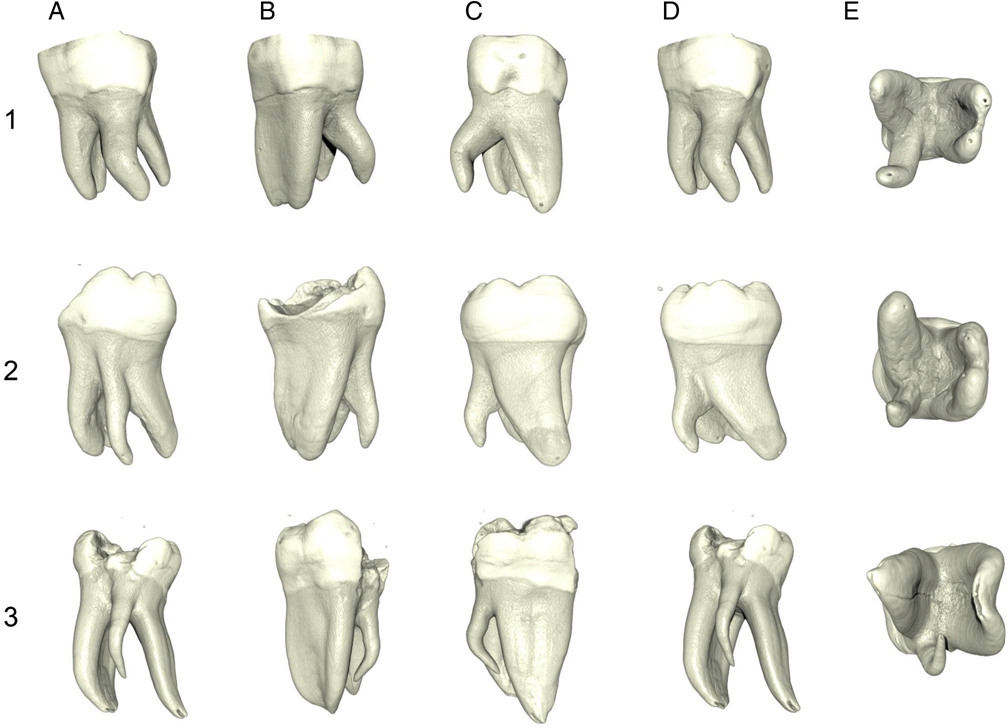
From a furcation view (E), it is possible to observe the curvature of the radix root with buccal orientation and the buccally displaced foramen location.
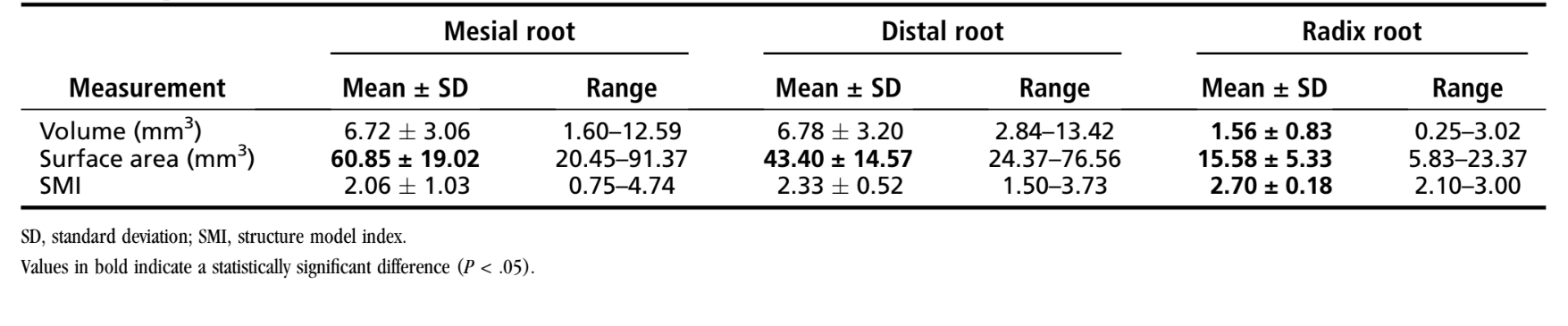
The 3D data are presented in Table 3. The radix canal showed a statistically significant difference from the mesial and distal root canals for all evaluated 3D morphometric data (P < .05). The SMI results showed that the radix canals presented a more cylindric geometry (2.70 ± 0.18) than the canals of the mesial and distal roots, which exhibited a more conic geometry (2.06 ± 1.03 and 2.33 ± 0.52, respectively).
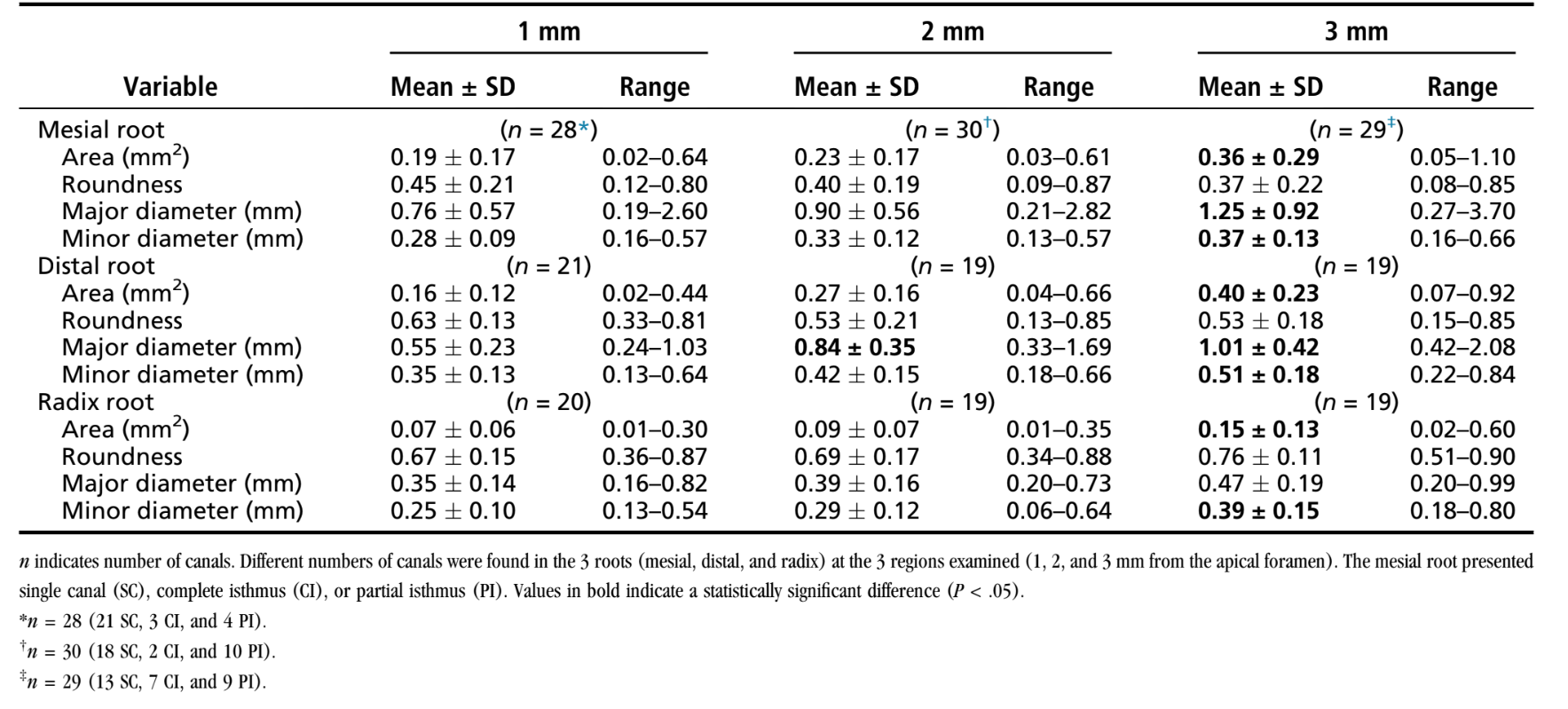
The morphometric 2D data recorded for the canals of each root at 1, 2, and 3 mm from the apical foramen are presented in Table 4. The 2D analysis revealed that the area increased gradually in the apex-crown direction in all root canals. Canal shape (roundness) in the radix root canal presented higher values compared with the mesial and distal root canals in the apical 3 mm (P < .05), with the mean value ranging from 0.67 ± 0.15 to 0.76 ± 0.11, which suggests a more round shape of the radix root canals. There was a significant difference between the major and minor diameters in the canals of the 3 roots, but this difference was greater in the mesial roots because they presented more flattened canals. Regarding the diameters of the radix root canals, the mean size of the minor diameter at 1 mm short of the foramen was 0.25 ± 0.10 mm.
Discussion
The presence of a third root in mandibular first molars has clinical implications in endodontic treatment. The identification of this additional root avoids missing a canal, which could lead to complications and treatment failure.
Although Walker and Quackenbush reported a 90% precision in the diagnosis of 3-rooted molars using only panoramic radiographs, the fact that the supernumerary (separate) root is found mainly in the same buccolingual plane of the distobuccal root may cause superimpositions on the preoperative radiographic image, resulting in inaccuracy in revealing this anatomic variation. In addition, a limitation of conventional images is to compress 3D anatomy into a 2D image or shadowgraph. In an attempt to overcome the drawbacks of radiographs for detecting the presence of a third root in mandibular first molars, it is helpful taking additional exposures changing the horizontal angulation of the main x-ray beam. This is particularly interesting in certain populations with Mongoloid traits in which the presence of a third root is considered as a normal morphologic variant. However, even multiple intraoral radiographs do not ensure the identification of all relevant anatomic variations of the teeth.
Cone-beam computed tomographic (CBCT) imaging is a useful imaging resource because 3D radiographic exposures allow for visualizing a new dimension and eliminate superimpositions. CBCT imaging provides additional information for diagnosis and therefore enables a more predictable management of complex endodontic conditions compared with intraoral radiographs alone. However, adherence to the ‘‘as low as reasonably achievable’’ concept is strongly recommended when selecting the appropriate radiographic imaging technique for each situation, which means that every radiation exposure should be justified clinically and principles should be followed to minimize patient exposure to ionizing radiation while maximizing the diagnostic benefit. Therefore, although CBCT imaging accurately displays complex dental anatomy, it should not be routinely used simply to search for a supernumerary root in mandibular first molars given the incidence of this variation is <5% in several populations.
Most studies evaluating 3-rooted mandibular first molars used periapical radiography as the study methodology mainly to collect information on the prevalence of the radix in different populations, its frequency in sexes, and the existence of bilateral symmetry. However, no relevant quantitative information has been provided for the planning of endodontic treatment in teeth with this anatomic variation.
MCT imaging has been widely used in different dental groups for different types of analyses of the internal and external dental morphology and anatomy. Compared with the traditional clearing and radiographic techniques, mCT scanning provides a more accurate examination of RCS configuration, allowing for a qualitative analysis of 3D models and a quantitative analysis of several geometric parameters. So far, this method has been used for the evaluation of 3-rooted mandibular first molars only in a 3-part study.
Little information is available on the mean length of radix roots. Chen et al used the lowest level of the distal furcation region as an anatomic landmark for the measurement and found values ranging from 3.59–10.07 mm. In the present study, the radix was measured from the cementoenamel junction toward the apex, reaching a mean size of 7.65 ± 1.55 mm. In both studies, the additional root was smaller than the mesial and distal roots, which is a clinically important factor to be considered.
In the present study, the analysis of 3D morphologic data (Table 3) revealed that the radix was thinner than the other roots, and the 2D data (Table 4) showed a mean apical canal diameter of 0.25 mm. These findings deserve attention as far as the biomechanical preparation of these canals is concerned because an effective disinfection of the RCS requires the removal of 150 to 200 mm of dentin. Therefore, although it is not yet feasible to have all teeth with a radix root examined by a high-quality 3D imaging method such as mCT imaging, as a routine approach in clinical settings, the publication of microtomographic data of root canal morphology obtained in laboratory studies, such as the present one, could increase significantly the safety and efficiency of root canal preparation procedures. Microtomographic studies in extracted 3-rooted mandibular molars add valuable information to clinical endodontists regarding the description of root morphology and canal geometry and the possible changes to be made in shaping procedures in order to adjust to the design of commercially available endodontic instruments. Most radix roots present, in a proximal perspective, a severe curvature with buccal orientation starting from the coronal third, which has been previously reported and can be observed in Figure 2. On the other hand, endodontic instruments are made from straight metal blanks and have a tendency of straightening the root canal during preparation, possibly resulting in instrument breakage and procedural errors such as ledges, zips, elbows, canal transportation, loss of working length, and root perforations. These aberrant results of root canal shaping make it difficult for endodontists to remove infected tissue remnants and achieve an adequate root canal seal and consequently may increase the risk for endodontic treatment failure.
In most teeth in the present study, the radix was observed in a distolingual position. The position of the radix canal orifice reflects directly on the shape of the access cavity of the mandibular first molar, so the modification to a trapezoidal shape extending distolingually, as seen in Figure 3, is essential to facilitate the localization and the access to the canal. Variations of the internal dental anatomy, such as projections, isthmuses, ramifications, and curvatures, challenge the root canal preparation and increase the risk of accidents. In accordance with previous reports, it was also observed that the radix canal orifice is usually covered by a dentin projection (Fig. 1), making its location even more difficult. Clinically, resources such as a microscope and ultrasound may be excellent adjuncts to access surgery, allowing for a precise identification and localization of the supernumerary root. When the radix canal orifice is located, the creation of a straight line access is of utmost importance because most radix roots are severely curved.
In view of the issues discussed previously, knowing the morphologic characteristics of radix roots is important to guide the planning of surgical and nonsurgical endodontic treatment in 3-rooted teeth and minimize the risks of complications during root canal preparation, making the treatment more predictable.
Conclusion
The presence of a supernumerary third root in mandibular first molars is an important and challenging anatomic variation, which the endodontist should be prepared to recognize. In general, the radix presents as a severely curved root with a predominantly distolingual location and a thin root canal with difficult access.
Authors: Luis Eduardo Souza-Flamini, Graziela Bianchi Leoni, Jardel Francisco Mazzi Chaves, Marco Aurélio Versiani, Antônio Miranda Cruz-Filho, Jesus Djalma Pécora, Manoel Damiaõ Sousa-Neto
References:
- Schilder H. Cleaning and shaping the root canal. Dent Clin North Am 1974;18: 269–96.
- Versiani MA, P´ecora JD, Sousa-Neto MD. The anatomy of two-rooted mandibular canines determined using micro-computed tomography. Int Endod J 2011;44:682–7.
- Versiani MA, Pécora JD, Sousa-Neto MD. Microcomputed tomography analysis of the root canal morphology of single-rooted mandibular canines. Int Endod J 2013;46:800–7.
- Siqueira JF, Alves FR, Versiani MA, et al. Correlative bacteriologic and micro- computed tomographic analysis of mandibular molar mesial canals prepared by self-adjusting file, Reciproc, and Twisted File systems. J Endod 2013;39:1044–50.
- Hargreaves KM, Cohen S, eds. Cohen’s Pathways of the Pulp, 10th ed. St Louis, MO: Elsevier; 2010.
- Vertucci F. Root canal morphology and its relationship to endodontic procedures. Endod Topics 2005;10:3–29.
- Carabelli G. Systematisches Handbuch der Zahnheilkunde, 2nd ed. Vienna, Austria: Braumuller and Seidel; 1844:114.
- De Moor RJ, Deroose CA, Calberson FL. The radix entomolaris in mandibular first molars: an endodontic challenge. Int Endod J 2004;37:789–99.
- Gulabivala K, Aung TH, Alavi A, Ng YL. Root and canal morphology of Burmese mandibular molars. Int Endod J 2001;34:359–70.
- Tu MG, Tsai CC, Jou MJ, et al. Prevalence of three-rooted mandibular first molars among Taiwanese individuals. J Endod 2007;33:1163–6.
- Chen G, Yao H, Tong C. Investigation of the root canal configuration of mandibular first molars in a Taiwan Chinese population. Int Endod J 2009; 42:1044–9.
- Huang RY, Cheng WC, Chen CJ, et al. Three-dimensional analysis of the root morphology of mandibular first molars with distolingual roots. Int Endod J 2010; 43:478–84.
- Versiani MA, Pécora JD, de Sousa-Neto MD. Flat-oval root canal preparation with self-adjusting file instrument: a micro-computed tomography study. J Endod 2011;37:1002–7.
- Versiani MA, Pécora JD, de Sousa-Neto MD. Root and root canal morphology of four-rooted maxillary second molars: a micro-computed tomography study. J Endod 2012;38:977–82.
- Leoni GB, Versiani M, Pecora J, Sousa-Neto M. Micro-computed tomography analysis of the root canal morphology of mandibular incisors. J Endod 2013;39: 1529–33.
- Gu Y, Lu Q, Wang H, et al. Root canal morphology of permanent three-rooted mandibular first molars–part I: pulp floor and root canal system. J Endod 2010; 36:990–4.
- Gu Y, Lu Q, Wang P, Ni L. Root canal morphology of permanent three-rooted mandibular first molars: Part II–measurement of root canal curvatures. J Endod 2010;36:1341–6.
- Gu Y, Zhou P, Ding Y, et al. Root canal morphology of permanent three-rooted mandibular first molars: Part III–An odontometric analysis. J Endod 2011;37: 485–90.
- Weller RN, Niemczyk SP, Kim S. Incidence and position of the canal isthmus. Part 1. Mesiobuccal root of the maxillary first molar. J Endod 1995;21:380–3.
- Calberson FL, De Moor RJ, Deroose CA. The radix entomolaris and paramolaris: clinical approach in endodontics. J Endod 2007;33:58–63.
- Walker RT, Quackenbush LE. Three-rooted lower first permanent molars in Hong Kong Chinese. Br Dent J 1985;159:298–9.
- Abella F, Mercadé M, Duran-Sindreu F, Roig M. Managing severe curvature of radix entomolaris: three-dimensional analysis with cone beam computed tomography. Int Endod J 2011;44:876–85.
- Yang Y, Zhang LD, Ge JP, Zhu YQ. Prevalence of 3-rooted first permanent molars among a Shanghai Chinese population. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010;110:e98–101.
- Patel S, Dawood A, Ford TP, Whaites E. The potential applications of cone beam computed tomography in the management of endodontic problems. Int Endod J 2007;40:818–30.
- Tu MG, Huang HL, Hsue SS, et al. Detection of permanent three-rooted mandibular first molars by cone-beam computed tomography imaging in Taiwanese individuals. J Endod 2009;35:503–7.
- Garg AK, Tewari RK, Agrawal N. Prevalence of three-rooted mandibular first molars among Indians using SCT. Int J Dent 2013; http://dx.doi.org/10.1155/2013/183869 [Epub ahead of print].
- Wu MK, Barkis D, Roris A, Wesselink PR. Does the first file to bind correspond to the diameter of the canal in the apical region? Int Endod J 2002;35:264–7.
- Kunert GG, Camargo Fontanella VR, de Moura AA, Barletta FB. Analysis of apical root transportation associated with ProTaper Universal F3 and F4 instruments by using digital subtraction radiography. J Endod 2010;36:1052–5.
- Peters OA. Current challenges and concepts in the preparation of root canal systems: a review. J Endod 2004;30:559–67.
- Villas-Bôas MH, Bernardineli N, Cavenago BC, et al. Micro-computed tomography study of the internal anatomy of mesial root canals of mandibular molars. J Endod 2011;37:1682–6.
- Walia HM, Brantley WA, Gerstein H. An initial investigation of the bending and torsional properties of Nitinol root canal files. J Endod 1988;14:346–51.
- Gu L, Wei X, Ling J, Huang X. A microcomputed tomographic study of canal isthmuses in the mesial root of mandibular first molars in a Chinese population. J Endod 2009;35:353–6.