
Micro–computed Tomographic Analysis of the Root Canal Morphology of the Distal Root of Mandibular First Molar
Abstract
Introduction: The aim of this study was to evaluate the morphologic aspects of the root canal anatomy of the distal root of a mandibular first molar using micro– computed tomographic analysis.
Methods: One- hundred distal roots of mandibular first molars were scanned using a micro–computed tomographic device at an isotropic resolution of 19.6 mm. The percentage frequency distribution of the morphologic configuration of the root canal was performed according to the Vertucci classification system. Two-dimensional parameters (area, perimeter, roundness, aspect ratio, and major and minor diameters) and the cross-sectional shape of the root canal were analyzed in the apical third at every 1-mm interval from the main apical foramen in roots presenting Vertucci types I and II configurations (n = 79). Data were statistically compared using the Kruskal-Wallis and Dunn tests with a significance level set at 5%.
Results: Seventy-six percent of the distal roots had a single root canal. Two, three, and four canals were found in 13%, 8%, and 3% of the sample, respectively. In 13 specimens, the configuration of the root canal did not fit into Vertucci’s classification. Overall, 2-dimensional parameter values significantly increased at the 3-mm level (P < .05). The prevalence of oval canals was higher at the 1-mm level and decreased at the 5-mm level in which long oval and flattened canals were more prevalent.
Conclusions: The distal roots of the mandibular first molars showed a high prevalence of single root canals. The prevalence of long oval and flattened canals increased in the coronal direction. In 13% of the samples, canal configurations that were not included in Vertucci’s configuration system were found. (J Endod 2015;■:1–6)
The knowledge of the anatomy of the root canal system and its variations play an important role in all steps of endodontic treatment. Therefore, the clinician should be able to fully understand the configuration of the root canal, aiming to choose the most appropriate treatment protocol and thereby increasing its success rate.
Generally, the morphology of the root canal varies greatly in shape and transversal cross-sections in different groups of teeth. In the posterior teeth, the mandibular first molar is recognized as exhibiting a complex and distinct range of variations in the morphology of the root canal system. This tooth usually has 2 roots, but, occasionally, it has 3, with 2 or 3 canals in the mesial root and 1, 2, or 3 canals in the distal root. When only 1 distal canal is present, it is usually oval-shaped buccolingually, and untreated surface areas were shown to be as high as 59%–79% when rotary instruments were used for the shaping procedure.
Micro–computed tomographic (micro-CT) imaging systems are currently being used for the ex vivo study of dental anatomy because they can provide a detailed quantitative and qualitative description of the external and internal anatomy of the teeth, overcoming the limitations of previous methods. Despite the fact that a considerable amount of information is available regarding the effect of endodontic procedures on the distal canals of mandibular molars, the literature lacks a detailed description of their anatomic configuration using new imagery technology. Thus, the aim of this study was to evaluate the morphologic aspects of the root canal anatomy of the distal roots of mandibular first molars using micro-CT technology.
Materials and Methods
One-hundred extracted 2-rooted mandibular first molars with fully formed apices collected from a Brazilian population were selected based on the appearance of crown morphology. Adherent soft tissue was removed by immersion in 2.5% sodium hypochlorite for 30 minutes. The teeth were then washed under tap water for 30 minutes and stored in 0.1% thymol solution. Patient, sex, and age were unknown. After ethics committee approval (protocol #131-2010), the teeth were mounted on a custom attachment and scanned in a micro-CT device (SkyScan 1174v2; Bruker-microCT, Kontich, Belgium) using 50 kV, 800 mA, a rotation step of 0.8, 360◦ of rotation, and an isotropic resolution of 19.6 mm. Images of each specimen were reconstructed from the apex to the level of the cementoenamel junction with dedicated software (NRecon v.1.6.9, Bruker-microCT), providing axial cross-sections of the inner structure of the sample.
Qualitative Analysis
Three-dimensional (3D) models of the dentin and root canals were reconstructed from the source images by using an automatic segmentation threshold and surface modeling with CTAn v.1.13 software (Bruker-microCT). CTVol v.2.2.1 and Data Viewer v.1.5 software (Bruker-microCT) were used for visualization and qualitative evaluation of the root canal configuration.
Quantitative Analysis
Two-dimensional (2D) evaluation (area, perimeter, roundness, major diameter, minor diameter, and aspect ratio) of the canal in the apical third at every 1-mm interval from the apical foramen to the 5- mm level was performed with CTAn v.1.13 software. These parameters were measured only in the distal roots presenting 1 canal at the apical third (n = 79). The area and perimeter were calculated using the Pratt algorithm. The cross-sectional appearance, round or more ribbon shaped, was expressed as roundness. The roundness of a discrete 2D object is defined as 4.A/(p.[dmax]2), where A is the area and dmax is the major diameter. The value of roundness ranges from 0 to 1, with 1 expressing the perfect circle. The major diameter was defined as the distance between the 2 most distant pixels in that object. The minor diameter was defined as the longest chord through the object that can be drawn in the orthogonal direction to that of the major diameter. The aspect ratio is a measure of shape, and it is achieved by dividing the value of the major diameter by the minor diameter. An oval canal has an aspect ratio higher than 1 and lower than 2, a long oval canal higher than 2 but lower than 4, and a flattened canal higher than 4. Root canals with aspect ratios lower than 1 were classified as nonoval. The prevalence of oval, long oval, and flattened root canals was expressed in percentages.
Statistical Analysis
Because the normality assumptions could not be verified (Shapiro-Wilk test, P < .05), the results of the 2D analysis, described as median values and interquartile ranges, were statistically compared using the Kruskal-Wallis and Dunn tests (Prisma 5.0 software; GraphPad Software Inc, La Jolla, CA) with a significance level set at 5%.
Results
Qualitative Analysis
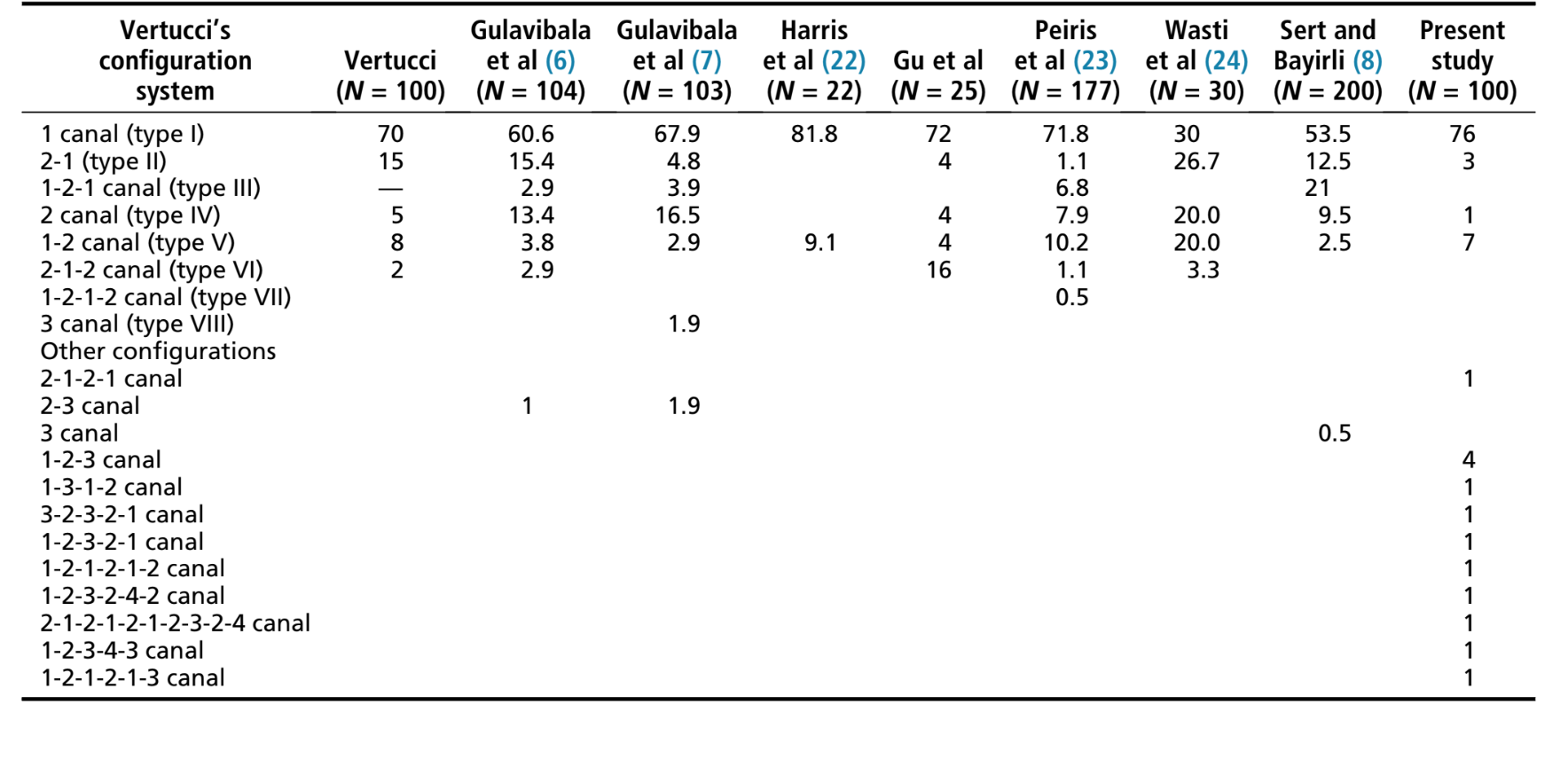
Table 1 shows the percentage frequency distribution of the morphologic configurations of the root canal observed in the distal roots of the mandibular first molars. The analysis of the 3D models of the root canal system showed that most of the specimens (76%) had a single root canal (Vertucci type I). A total of 2, 3, and 4 canals were observed in 13%, 8%, and 3% of the sample, respectively. A single canal leaving the chamber and dividing into 2 canals at the apex (Vertucci type V) and 2 separate canals leaving the chamber but merging short of the apex to form a single canal (Vertucci type II) were observed in 7 and 3 specimens, respectively. Only 1 specimen showed 2 distinct canals from the pulp chamber to the apex (Vertucci type IV). In 13 specimens, canal configurations that were not included in the Vertucci configuration system were found. Figure 1A–N shows representative 3D models of the configuration system of the distal canals of mandibular first molars.

Quantitative Analysis
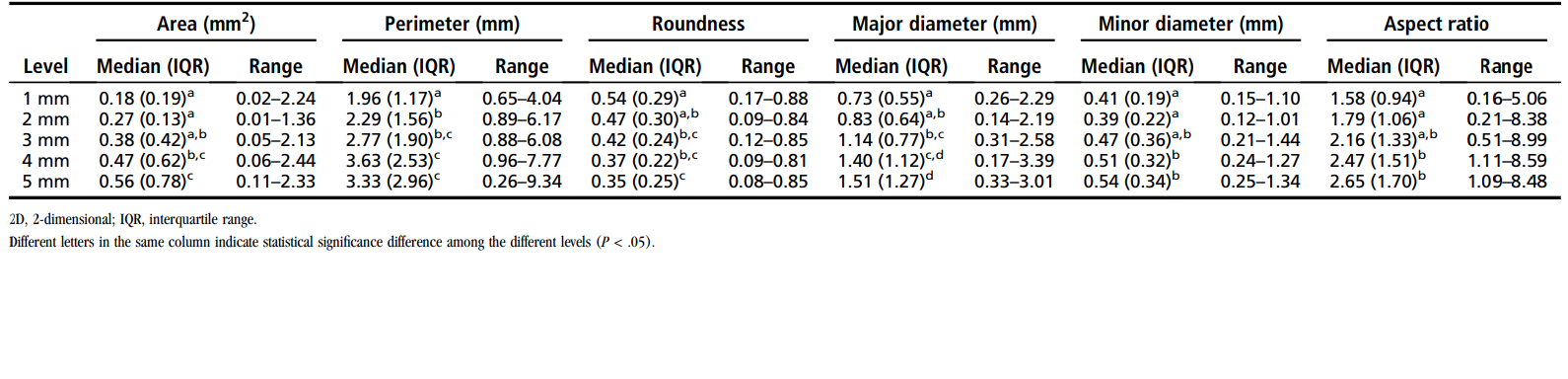
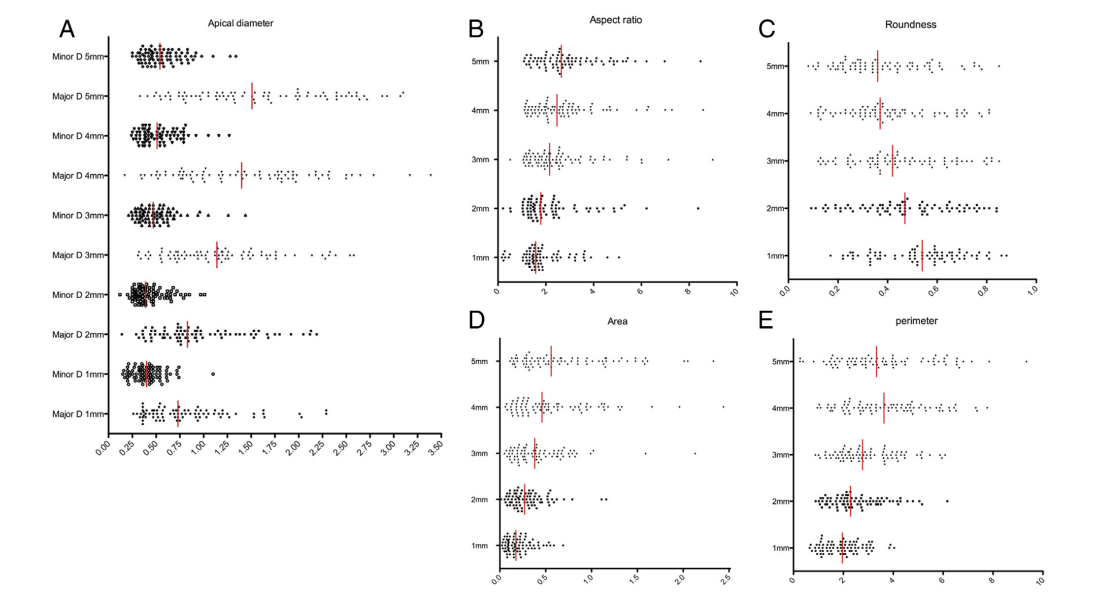
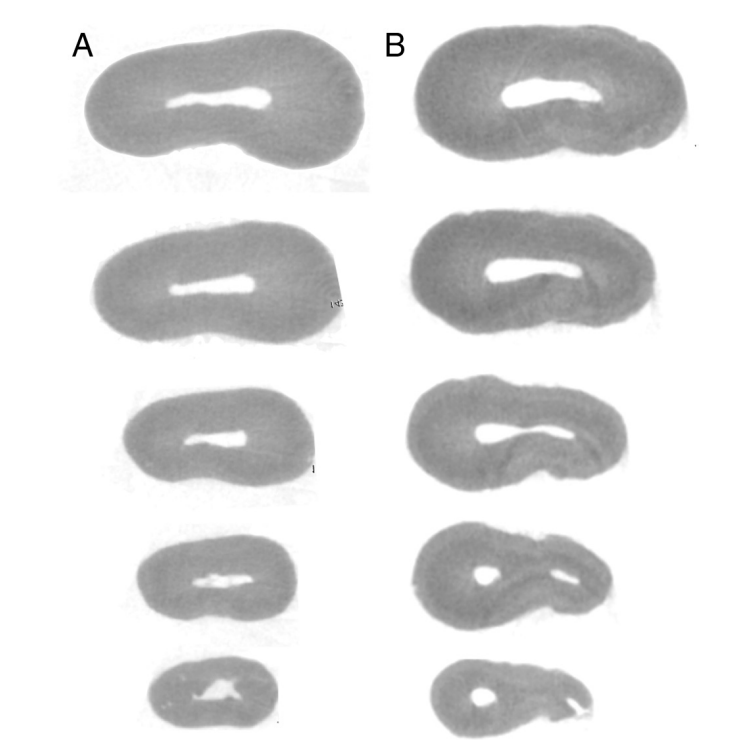
The morphometric measurements were performed in 79 specimens presenting a single canal at the apical third and classified as Vertucci types I (n = 76) and II (n = 3). The results of the 2D analyses of the root canal at the apical third are detailed in Table 2 and Figure 2A–E. Area, perimeter, and major and minor diameter values significantly decreased toward the apex (P < .05). The root canal shape did not remain constant from 1 level to the next. The median values of roundness and aspect ratio indicated a prevalence of oval-shaped canals in the last 2 mm and long oval-shaped canals at the 3-, 4-, and 5-mm levels (Tables 2 and 3). Representative cross-sections of the more prevalent anatomies are shown in Figure 3A and B.
Discussion
In 1984, Vertucci classified the root canal anatomy into 8 different configurations after the study of 2400 cleared teeth. Several studies on the distal roots of mandibular molars attempted to classify the morphology of the root canal system using this configuration system. Table 1 summarizes the main results of these studies. Overall, the distal roots of mandibular first molars showed a high prevalence of a single canal (Vertucci type I configuration), as in the present study. Using conventional methods, the prevalence of a single canal in the distal root has been reported to range from 50% to 84%. To date, only 2 studies evaluated the anatomy of the distal roots of mandibular molars using micro-CT technology. According to these authors, single canals were found in 72% and 81% of the distal roots, which is similar to the present results (76%).
The second most frequent anatomic configuration of the distal root has been reported to be Vertucci type V, which is described as a single canal that leaves the chamber and divides into 2 canals at the apex. Vertucci type II and IV configurations were also reported as the second most prevalent anatomic variation in other studies; however, these configurations were observed in only 3% and 1% of the samples, respectively, in the present study. Additionally, although the presence of different root canal configurations in the distal canals of mandibular molars has been rarely reported, clinicians must be aware of these anatomic variations. In the present study, 13% of the sample showed canal configurations that were not included in the Vertucci configuration system.
It is noteworthy that the wide range of variation reported in the literature, regarding the prevalence of different configuration systems in the same group of teeth, can probably be related to the methodology involved such as clearing, cross-section, or micro-CT system; the different number of the sample selection; or ethnic differences. As a result, the micro-CT method has been considered the most accurate tool for the identification of fine anatomic structures, which may explain the considerable amount of anatomic variations found in this study.
Algorithms used in micro-CT technology have also been used for the study and morphometric description of the root canal space, allowing further measurement of basic 2D geometric parameters such as area, perimeter, roundness, and major and minor diameters. When comparing the 2D results of this study with the available micro-CT data in other groups of teeth, it can be observed that the area in the last apical millimeter of the distal root canal (0.18 mm2) was similar to mandibular canines (0.20 mm2) but higher than mandibular incisors (0.07 mm2). At the apical level, the major diameter values (0.73 mm) were found to be higher than in the mandibular canines (0.59 mm) and mandibular incisors (0.44 mm), whereas roundness was similar for the mandibular incisors (0.54 at the 1-mm level and 0.35 at the 5-mm level). In this study, it should be pointed out that the major apical diameter values were higher than the ones previously reported by Wu et al and Harris et al. Such differences could be explained through the diversity in the sample size and evaluation methods.
Effective root canal cleaning relies on accurate determination of the working length and adequate apical canal enlargement, which allow for a better distribution of root canal irrigants in the apical and isthmuses areas, optimizing the root canal decontamination process. Another important topic related to the cleaning and shaping procedures is the cross-sectional geometric appearance of the root canal. Despite the presence of a single canal in 76% of the samples (Vertucci type I), the percentage of oval and long oval canals at the apical third was high (64% and 25%, respectively), as shown by the aspect ratio values.
Previous researchers have reported that the percentage of uninstrumented surface canal areas in the distal roots of mandibular molars after the use of rotary instruments ranged from 59%–79% (11) and 23% when the Self-Adjusting File (ReDent-Nova, Ra’anana, Israel) was used (20). These high percentages of uninstrumented areas were associated with the cross-section and cinematics of rotary instruments and/or the presence of a large apical diameter, especially in the buccolingual direction of the distal canals. In this situation, recesses in oval-shaped canals may not be included in the rounded preparation created by the rotation of instruments and, thus, remain unprepared. This information suggests that an ideal cleaning and shaping technique should be focused on the enlargement of the distal root canals of mandibular molars, mostly in the buccolingual direction, preserving the amount of remaining dentin in the mesiodistal direction.
Another remarkable point was the increased prevalence of flattened canals observed in a coronal direction from the apex. As shown in Figure 2, a significant amount of the distal canals showed an increase in the aspect ratio (>4) and a decrease in the roundness values, especially at the 4- and 5-mm levels from the foramen. It suggests that, in a considerable amount of cases, the single root canal may need to be prepared considering the buccal and lingual aspects as 2 individual canals.
Despite the fact that the distal root canals of mandibular first molars do not usually present abrupt curvatures or lower apical diameters in comparison with the mesial root, the complexity of its cross-section and the considerable amount of anatomic variations show that efforts to improve the mechanical preparation and irrigation of uninstrumented recesses need to be considered. Although the main canal is usually incorporated during the shaping process, tissue remnants, hard tissue debris, and even bacteria frequently remain unaffected by the instrumentation process because of the intrinsic physical limitations of the instruments. To avoid such limitations and make endodontic treatment more predictable, the use of magnification and methods that allow the proper distribution of root canal irrigants and the elimination of accumulated hard tissue debris is of the utmost importance during the cleaning and shaping process. In summary, the reported data may help clinicians understand the variations in the root canal morphology of the distal roots of mandibular first molars in order to overcome problems associated with disinfection procedures.
Conclusions
The distal roots of mandibular first molars showed a high prevalence of single root canals. The prevalence of long oval and flattened canals increased in the coronal direction. In 13% of the samples, canal configurations that were not included in the Vertucci configuration system were found.
Authors: Carolina Filpo-Perez, Clovis Monteiro Bramante, Marcelo Haas Villas-Boas, Marco Antonio Húngaro Duarte, Marco Aurélio Versiani, Ronald Ordinola-Zapata
References:
- Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol 1984;58:589–99.
- Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endod Topics 2005;10:3–29.
- Jou YT, Karabucak B, Levin J, Liu D. Endodontic working width: current concepts and techniques. Dent Clin North Am 2004;48:323–35.
- Wu MK, R’Oris A, Barkis D, Wesselink PR. Prevalence and extent of long oval canals in the apical third. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000;89: 739–43.
- Versiani MA, Pécora JD, Sousa-Neto MD. Microcomputed tomography analysis of the root canal morphology of single-rooted mandibular canines. Int Endod J 2013;46:800–7.
- Gulabivala K, Aung TH, Alavi A, Ng YL. Root and canal morphology of Burmese mandibular molars. Int Endod J 2001;34:359–70.
- Gulabivala K, Opasanon A, Ng YL, Alavi A. Root and canal morphology of Thai mandibular molars. Int Endod J 2002;35:56–62.
- Sert S, Bayirli GS. Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endod 2004;30: 391–8.
- Villas-Boas MH, Bernardineli N, Cavenago BC, et al. Micro-computed tomography study of the internal anatomy of mesial root canals of mandibular molars. J Endod 2011;37:1682–6.
- Gu Y, Lu Q, Wang H, et al. Root canal morphology of permanent three-rooted mandibular first molars—part I: pulp floor and root canal system. J Endod 2010;36:990–4.
- Paqué F, Balmer M, Attin T, Peters OA. Preparation of oval-shaped root canals in mandibular molars using nickel-titanium rotary instruments: a micro-computed tomography study. J Endod 2010;36:703–7.
- Fumes AC, Sousa-Neto MD, Leoni GB, et al. Root canal morphology of primary molars: a micro-computed tomography study. Eur Arch Paediatr Dent 2014;15: 317–26.
- Leoni GB, Versiani MA, Pécora JD, Damião de Sousa-Neto M. Micro–computed tomographic analysis of the root canal morphology of mandibular incisors. J Endod 2014;40:710–6.
- Ordinola-Zapata R, Bramante CM, Villas-Boas MH, et al. Morphologic micro- computed tomography analysis of mandibular premolars with three root canals. J Endod 2013;39:1130–5.
- Versiani MA, P´ecora JD, de Sousa-Neto MD. Root and root canal morphology of four-rooted maxillary second molars: a micro-computed tomography study. J Endod 2012;38:977–82.
- Versiani MA, Cristescu RC, Saquy PC, et al. Enamel pearls in permanent dentition: case report and micro-CT evaluation. Dentomaxillofac Radiol 2013;42:20120332.
- Milanezi de Almeida M, Bernardineli N, Ordinola-Zapata R, et al. Micro-computed tomography analysis of the root canal anatomy and prevalence of oval canals in mandibular incisors. J Endod 2013;39:1529–33.
- Paes da Silva Ramos Fernandes LM, Rice D, Ordinola-Zapata R, et al. Detection of various anatomic patterns of root canals in mandibular incisors using digital periapical radiography, 3 cone-beam computed tomographic scanners, and micro- computed tomographic imaging. J Endod 2014;40:42–5.
- Lee KW, Kim Y, Perinpanayagam H, et al. Comparison of alternative image reformatting techniques in micro-computed tomography and tooth clearing for detailed canal morphology. J Endod 2014;40:417–22.
- Paqué F, Peters OA. Micro-computed tomography evaluation of the preparation of long oval root canals in mandibular molars with the Self-Adjusting File. J Endod 2011;37:517–21.
- Rechenberg DK, Paqué F. Impact of cross-sectional root canal shape on filled canal volume and remaining root filling material after retreatment. Int Endod J 2013;46: 547–55.
- Harris SP, Bowles WR, Fok A, McClanahan SB. An anatomic investigation of the mandibular first molar using micro-computed tomography. J Endod 2013;39: 1374–8.
- Peiris HR, Pitakotuwage TN, Takahashi M, et al. Root canal morphology of mandibular permanent molars at different ages. Int Endod J 2008;41:828–35.
- Wasti F, Shearer AC, Wilson NH. Root canal systems of the mandibular and maxillary first permanent molar teeth of south Asian Pakistanis. Int Endod J 2001;34:263–6.
- de Pablo OV, Estevez R, Péix Sánchez M, et al. Root anatomy and canal configuration of the permanent mandibular first molar: a systematic review. J Endod 2010;36: 1919–31.
- Rwenyonyi CM, Kutesa A, Muwazi LM, Buwembo W. Root and canal morphology of mandibular first and second permanent molar teeth in a Ugandan population. Odontology 2009;97:92–6.
- Versiani MA, Pécora JD, Sousa-Neto MD. The anatomy of two-rooted mandibular canines determined using micro-computed tomography. Int Endod J 2011;44: 682–7.
- Siqueira JF, Alves FR, Versiani MA, et al. Correlative bacteriologic and micro- computed tomographic analysis of mandibular molar mesial canals prepared by Self-adjusting File, Reciproc, and Twisted File systems. J Endod 2013;39:1044–50.
- Schäfer E, Diez C, Hoppe W, Tepel J. Roentgenographic investigation of frequency and degree of canal curvatures in human permanent teeth. J Endod 2002;28: 211–6.
- Nair PN, Henry S, Cano V, Vera J. Microbial status of apical root canal system of human mandibular first molars with primary apical periodontitis after ‘‘one-visit’’ endodontic treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;99: 231–52.