
Glide Path with Reciprocating Driven Pathfinding Instrument: Performance and Fracture Rate
Abstract
Introduction: This study assessed the number of mesial and distal canals of mandibular molars in which the R-Pilot pathfinding reciprocating instrument reached the working length (WL) during macro glide path procedure. Fracture and deformation rates were also evaluated. Methods: One hundred fifty-six root canals of 52 teeth were scouted to the length of the apical foramen. Then the R-Pilot instrument was positioned at the canal orifice and activated. The instrument was moved by using a pecking motion and light apical pressure. This procedure was repeated in an attempt to reach the WL. The type of fracture and/or instrument deformation was assessed by scanning electron microscopy, whereas the roots with fractured instruments were scanned through micro-computed tomography. The percentage frequency distribution of fractures, deformations, and root canals in which the R-Pilot reached the WL were recorded and statistically compared by using the Pearson’s χ2 test with α = 5%. Results: R-Pilot instruments reached the WL in 139 root canals (89.10%), and χ2 test showed a significant difference between the observed frequencies and the expected frequencies (χ2 = 95.41, P = .000). The observed frequencies of fractures (2.56%) and deformations (1.92%) were also significantly lower than the expected (fracture: χ2 = 140.41, P = .000; deformation: χ2 = 144.23, P = .000). Fractures occurred mostly at the apical and curved parts of the root canals. Conclusions: R-Pilot reached the WL in 89.10% of the root canals of mandibular molars with fracture and deformation rates of 2.56% and 1.92%, respectively. (J Endod 2020;1–5.)
Glide path has been defined as a clinical procedure to expand or create a smooth tunnel from the coronal portion of the root canal to its physiological terminus before its final enlargement, aiming to control the torsional stress and to reduce the odds of nickel-titanium (NiTi) instruments’ fracture. The essential steps that preceded the glide path have been referred to as “micro glide path” and comprise both canal scouting and apical patency (ie, the location of the main foramen exit); they are usually performed with small pre-curved stainless steel hand files and gentle watch-winding movements. However, these preliminary procedures can be challenging and time-consuming in clinics, especially when dealing with curved and/or calcified root canals. After micro glide path has been successfully accomplished, the already scouted canal still needs to be further enlarged, a procedure named “macro glide path”. This is performed by using either hand files or specially designed mechanically driven NiTi instruments; the latter is preferred once it has been associated with reduced postoperative pain and flare-ups, as well as better maintenance of the original canal anatomy. On the other hand, because the canal is still narrow, the use of rotary NiTi instruments with small dimensions, the so-called pathfinders, has been reported to be more susceptible to fracture and unpredictable in terms of clinical efficacy and safety. Aiming to overcome these drawbacks, several approaches have been proposed including changes in their NiTi alloy, design, and, more recently, the movement kinematics.
The reciprocating motion has raised new perspectives for mechanically activated preparation because it reduces the working time, the cyclic fatigue, and the torsional stress of instruments when compared with continuous rotation. Recently, the R-Pilot instrument (VDW GmbH, Munich, Germany) was launched for macro glide path preparation in reciprocating motion. R-Pilot is made from M-Wire NiTi alloy with 0.04 taper, S-shaped cross section, and a non-cutting tip with 0.125-mm diameter. Although its mechanical properties have been evaluated in previous studies, its performance for reaching the working length (WL) is still unknown. Therefore, the present study aimed to assess the fracture and deformation rates, as well as the number of root canals in which the R-Pilot instrument was able to reach the WL of mesial and distal canals of mandibular molars during macro glide path procedure.
The working hypotheses of this study were that the R-Pilot instruments reach the WL in a high frequency of cases and have low fracture/ deformation rates.
Materials and methods
Sample Size Estimation
On the basis of a study with similar experimental design, the effect size for using the reciprocating movement to reach the WL was determined to be 0.296. Therefore, using the χ2 family and the goodness of fit test (G*Power 3.1 for Macintosh; Heinrich Heine, Universität Düsseldorf, Düsseldorf, Germany) with additional parameters of alpha-type error of 0.05 and beta power of 0.95, a minimal sample size of 149 root canals was indicated.
Specimen Selection
After approval of this project by the local Ethics Committee (protocol no. 2.985.618), a total of 100 first and second mandibular molars, extracted for reasons not related to this study, were randomly selected from a pool of teeth, radiographed in mesial and distal directions by using a digital sensor (Schick CDR digital radiographic system; Dentsply Sirona, Charlotte, NC), and stored in 0.5% thymol solution at 5◦C. Teeth with open apex, resorptions, or root fractures were excluded. The inclusion criteria consisted of mandibular molars with moderately curved roots (10◦– 20◦), 2 independent mesial root canals, from its orifice level to its apical terminus, and 1 or 2 independent canals on the distal root. Afterwards, 52 mandibular molars with 156 root canals were selected.
Glide Path Preparation
After conventional access preparation, each tooth was mounted on a specific apparatus (IM Brazil, São Paulo, SP, Brazil) that simulates the alveolar socket and allows the connection of the metal lip clip of an electronic apex locator (EAL), according to a previous study. As recommended by the manufacturer, before the use of the R-Pilot instrument, root canal scouting (micro glide path) was performed with a 25-mm size .08 hand file (C-Pilot; VDW GmbH) connected to an EAL (Root ZX; J Morita USA Inc, Irvine, CA) by applying gentle to moderate pressure and careful watch- winding motions along the root canal until the EAL screen displayed the “0.0’’ reading mark. The WL was set as this reference point.
Before the macro glide path procedure, all selected R-Pilot instruments were inspected through an operative microscope at X16 magnification to exclude instruments with critical defects or distortions, and none were excluded. R-Pilot instrument was then mounted on a contra-angle handpiece (Sirona, Bensheim, Germany) powered by an electric motor (VDW Gold; VDW GmbH), and the file holder of the EAL was clipped to the nonactive part of the blade. After that, the R-Pilot was positioned at the orifice level with the same insertion angle of the scouting file until resistance was felt and activated in reciprocating motion (“RECIPROC ALL” mode). The instrument was moved to the apical direction using 3 in-and-out pecking motions of about 3 mm in amplitude with a light apical pressure, after which it was removed from the canal, cleaned with gauze moistened with alcohol, and inspected for fracture or deformation. The root canal was then irrigated with 2 mL of 2.5% sodium hypochlorite. This procedure was repeated 3 times in an attempt to reach the WL. After that, if the instrument did not reach the WL, this procedure was stopped.
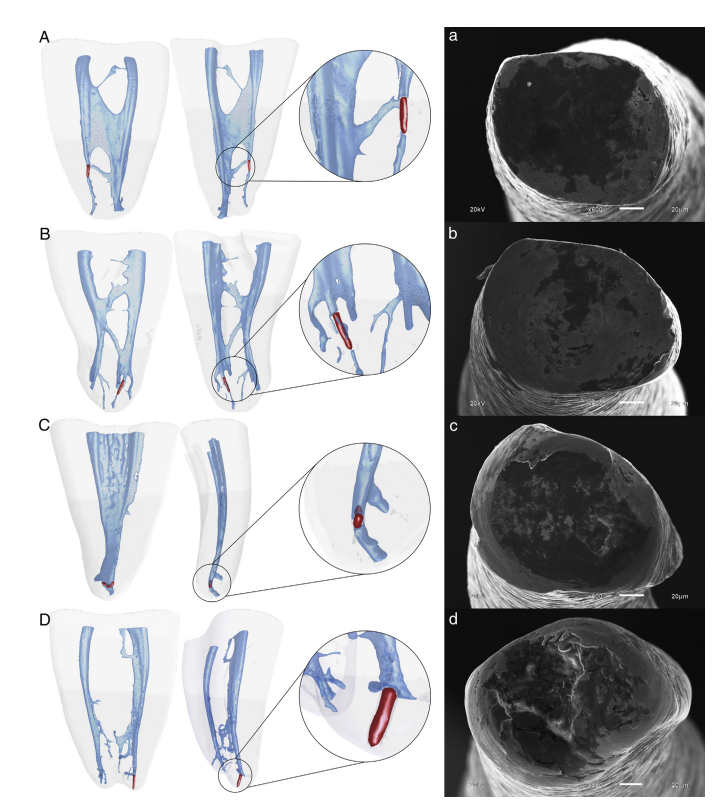
The numbers of fractures, deformations, and root canals in which the R-Pilot instrument reached the WL were recorded. The type of fracture and/or deformation was determined at X200 to X2000 magnifications through a scanning electron microscope (SEM) (JEOL JSM 6510 LV; JEOL, Tokyo, Japan) after the instruments were ultrasonically cleaned. In addition, roots with a fractured instrument were scanned in a micro-computed tomography (micro-CT) device (SkyScan 1173; Bruker microCT, Kontich, Belgium) operated at 80 kV and 100 mA, with an isotropic resolution of 12.82 mm, 360◦ rotation around the vertical axis, and rotation step of 0.4◦ to verify the possible reasons for the fracture (Fig. 1). A specialist in endodontics with 5 years of clinical experience performed all procedures, and each instrument was used in only 1 tooth and discarded.
Statistical Analysis
The percentage frequency distributions (%) of specimens in which the R-Pilot instrument reached and did not reach the WL were recorded and statistically compared by using the Pearson’s χ2 test. Alpha-type error and critical χ2 were set at 0.05 and 3.84, respectively, as indicated by the sample power calculation.
Results
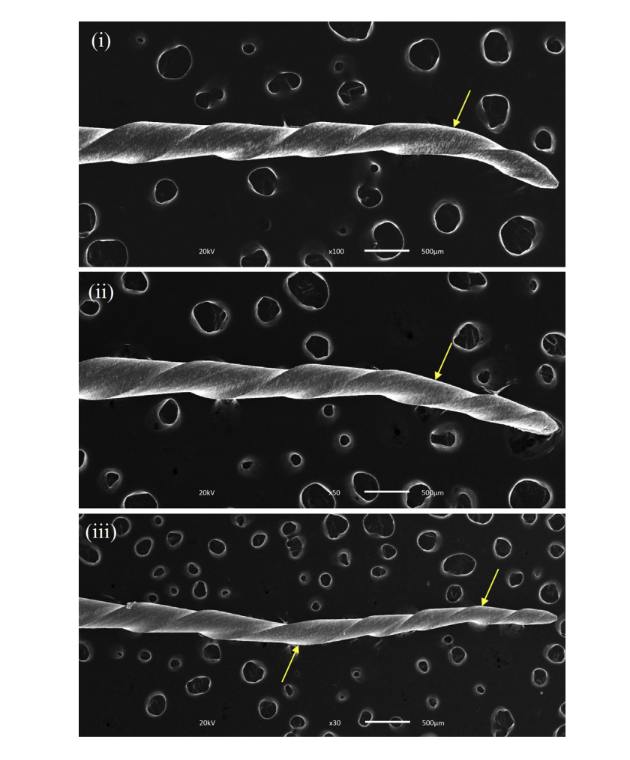
Overall, R-Pilot instruments reached the WL in 139 root canals (89.10%). The c2 test showed that the observed frequencies in which the R- Pilot reached the WL were significantly different from the expected frequencies (χ2 = 95.41, P = .000). During the experiment, fracture was observed in 4 instruments (2.56%) and classified as mixed (n = 3) and torsional (n = 1) (Fig. 1), whereas 3 instruments (1.92%) showed blade deformation (Fig. 2). Chi-square analysis demonstrated that the observed frequencies of fracture and deformation were also significantly lower than the expected (fracture: χ2 = 140.41, P = .000; deformation: χ2 = 144.23, P = .000). Figure 1 shows 3-dimensional (3D) models acquired by micro-CT scanning of the 4 roots depicting the fractured instruments located mostly at the apical part of the root, with sizes ranging from 0.67–0.85 mm.
Discussion
R-Pilot instruments reached the WL in 139 of 156 mesial and distal root canals (89.10%) of mandibular molars, with a low percentage frequency of fracture and deformation. Thus, the working hypotheses of this study were confirmed. The present results are somewhat interesting, particularly when compared with the ability of rotary-driven pathfinding instruments to reach the apical foramen (38.30%–68.30%). The present findings can be explained by 3 main reasons:
- the asymmetric reciprocating kinematics that maintains the apical progression of the instrument while reducing torsional stress,
- the design of the instrument, with a small tip diameter (0.125 mm) and a constant taper (0.04 mm), that minimizes its contact with the dentinal walls, and
- the S-shaped cross section, which provides an effective cutting efficiency.
During major glide path preparation, the pathfinding instrument is exposed to a mechanical stress and may fracture by torsional or cyclic fatigue. Because pathfinding instruments are more flexible because of their smaller dimensions, cyclic fatigue appears to be less relevant than torsional stress as the cause of instrument fracture. In the present study, very low fracture (2.56%) and deformation (1.92%) rates were observed, and the correlative imaging approach used allowed for a qualitative understanding of the reasons for instrument failure. The fractured instruments were evaluated under SEM analysis, and the 4 roots with R-Pilot fragments were scanned in a micro-CT device. SEM analysis demonstrated mixed fracture types in 3 instruments and torsional failure in another instrument (Fig. 1), whereas the analysis of the 3D models showed that 2 of the roots had relatively straight but narrow root canals, and fracture occurred at the middle (n = 1) and apical (n = 1) thirds, whereas the other instruments fractured at the curvature of the apical canal (Fig. 1). It may be assumed that the incidence of a single torsional fracture type would be as a consequence of the reciprocating movement, which efficiently avoided the taper lock phenomenon that often occurs under continuous rotation. On the other hand, the mixed fractures were possibly related to the operator. Advancing this type of instrument toward the apex is somewhat difficult, and it is not unusual for an operator to increase the pressure on it, causing its bending because of its low taper and small core. Taken together, the increased flexion, the binding of the tip, and the apical curvature were possibly the cause of the mixed fractures.
Several studies have shown the efficacy of EALs, demonstrating that the electronic method is the best way to a correct WL determination. In addition, the Root ZX is usually considered as the gold standard EAL. The EAL reading of 0.0 mark is relevant because it shows the determination of the major apical foramen. Thus, in this study, the 0.0 reading mark of the Root ZX was used as the reference point to evaluate the R-Pilot instrument’s performance.
In comparative studies, it is extremely important to standardize the sample to avoid bias related to the root canal morphology. However, the present investigation was not a comparative study. Therefore, root canals with moderate curvature were selected considering their high incidence in mandibular molars and because they represent a clinical challenge to perform glide path procedures. All root canals were apparently negotiable, because scouting was successfully performed with a .08 hand file. It means that no significant anatomic challenges could be regarded as the main cause of the R-Pilot instruments that did not reach the WL. It is possible that dentinal debris created during glide path management was packed into the apical canal, preventing the instruments from reaching the foramen, which only emphasizes the importance of root canal irrigation; however, this remains to be proven in further studies.
The evaluation of the percentage frequency that pathfinding instruments reached the WL without breakage or distortion seems to be the best method to rank their performance and safety. In this sense, the methodology applied to this study fits very well into this purpose. It is also important to highlight that in the study of the frequency of a given event in a population, a control group is not necessarily required. For instance, in the present study, a χ2 statistical procedure adequately certifies the significance of the observed frequencies. Thus, the nature of the present study was not comparative, and no reference group was needed because the main purpose was limited to observe the performance of R-Pilot instruments, the first reciprocating pathfinder launched in the market. This point may be considered as a limitation of this study, but the large sample size required to obtain a reliable performance profile of a given instrument may be taken into consideration. Therefore, further studies using the proposed method are needed to evaluate the performance of newer reciprocating driven pathfinder instruments.
Conclusions
Under the conditions of the present study, it can be concluded that R-Pilot instruments reached the WL in 89.10% of previously scouted mesial and distal canals of mandibular molars with fracture and deformation rates of 2.56% and 1.92%, respectively.
Authors: Gustavo De-Deus, Milla Lessa Cardoso, Marco Simões-Carvalho, Emmanuel J. N. L. Silva, Felipe Gonçalves Belladonna, Daniele Moreira Cavalcante, Diogo da Silva Oliveira, Erick Miranda Souza, Ricardo Tadeu Lopes, Marco Aurélio Versiani
References:
- West JD. The endodontic Glidepath: “secret to rotary safety”. Dent Today 2010;29:90–3.
- Ruddle CJ, Machtou P, West D. Endodontic canal preparation: new innovations in glide path management and shaping canals. Dent Today 2014;33:1–7.
- Van der Vyver PJ. Creating a glide path for rotary NiTi instruments: part one. Int Dent J 2010;13:6–10.
- Van der Vyver PJ. ProGlider™: clinical protocol. Endod Practice 2014;7:42–7.
- Jonker CH, Van der Vyver PJ, De Wet FA. The influence of glide path preparation on the failure rate of WaveOne reciprocating instruments. SADJ 2014;69:266–9.
- Berutti E, Negro AR, Lendini M, Pasqualini D. Influence of manual preflaring and torque on the failure rate of ProTaper rotary instruments. J Endod 2004;30:228–30.
- Patiño PV, Biedma BM, Li´ebana CR, et al. The influence of a manual glide path on the separation rate of NiTi rotary instruments. J Endod 2005;31:114–6.
- Pasqualini D, Bianchi CC, Paolino DS, et al. Computed micro-tomographic evaluation of glide path with nickel-titanium rotary PathFile in maxillary first molars curved canals. J Endod 2012;38:389–93.
- Berutti E, Cantatore G, Castellucci A, et al. Use of nickel-titanium rotary PathFile to create the glide path: comparison with manual preflaring in simulated root canals. J Endod 2009;35:408–12.
- De-Deus G, Belladonna FG, Souza EM, et al. Scouting ability of 4 pathfinding instruments in moderately curved molar canals. J Endod 2016;42:1540–4.
- Pasqualini D, Mollo L, Scotti N, et al. Postoperative pain after manual and mechanical glide path: a randomized clinical trial. J Endod 2012;38:32–6.
- Elnaghy AM, Elsaka SE. Evaluation of root canal transportation, centering ratio, and remaining dentin thickness associated with ProTaper Next instruments with and without glide path. J Endod 2014;40:2053–6.
- Arias A, Singh R, Peters OA. Differences in torsional performance of single-use and multiple- instrument rotary systems for glide path preparation. Odontology 2016;104:192–8.
- Grande NM, Ahmed HM, Cohen S, et al. Current assessment of reciprocation in endodontic preparation: a comprehensive review—part I: historic perspectives and current applications. J Endod 2015;41:1778–83.
- Plotino G, Ahmed HM, Grande NM, et al. Current assessment of reciprocation in endodontic preparation: a comprehensive review—part II: properties and effectiveness. J Endod 2015;41:1939–50.
- Keskin C, _Inan U, Demiral M, Kelesx A. Cyclic fatigue resistance of R-Pilot, WaveOne Gold Glider, and ProGlider glide path instruments. Clin Oral Invest 2018;22:3007–12.
- Özyürek T, Uslu G, Gündoğar M, et al. Comparison of cyclic fatigue resistance and bending properties of two reciprocating nickel-titanium glide path files. Int Endod J 2018;51:1047–52.
- Topçuoğlu HS, Topçuoğlu G, Kafdağ Ö, Arslan H. Cyclic fatigue resistance of new reciprocating glide path files in 45- and 60-degree curved canals. Int Endod J 2018;51:1053–8.
- Yılmaz K, Uslu G, Gündoğar M, et al. Cyclic fatigue resistances of several nickel-titanium glide path rotary and reciprocating instruments at body temperature. Int Endod J 2018;51:924–30.
- Santos CB, Simões-Carvalho M, Perez R, et al. Torsional fatigue resistance of R-Pilot and WaveOne Gold Glider NiTi glide path reciprocating systems. Int Endod J 2019;52:874–9.
- Sung SY, Ha JH, Kwak SW, et al. Torsional and cyclic fatigue resistances of glide path preparation instruments: G-file and PathFile. Scanning 2014;36:500–6.
- Gambarini G, Plotino G, Sannino GP, et al. Cyclic fatigue of instruments for endodontic glide path. Odontology 2015;103:56–60.
- Martins JNR, Marques D, Mata A, Carame^s J. Clinical efficacy of electronic apex locators: systematic review. J Endod 2014;40:759–77.
- Tsesis I, Blazer T, Ben-Izhack G, et al. The precision of electronic apex locators in working length determination: a systematic review and meta-analysis of the literature. J Endod 2015;41:1818–23.
- Stöber EA, Duran-Sindreu F, Mercadé M, et al. An evaluation of Root ZX and iPex apex locators: an in vivo study. J Endod 2011;37:608–10.