
A new system for classifying root and root canal morphology
Abstract
Knowledge of root and root canal morphology is a pre-requisite for effective nonsurgical and surgical endodontic treatments. The external and internal morphological features of roots are variable and complex, and several classifications have been proposed to define the various types of canal configurations that occur commonly. More recently, improvements in nondestructive digital image systems, such as cone-beam and micro-computed tomography, as well as the use of magnification in clinical practice, have increased the number of reports on complex root canal anatomy. Importantly, using these newer techniques, it has become apparent that it is not possible to classify many root canal configurations using the existing systems. The purpose of this article is to introduce a new classification system that can be adapted to categorize root and root canal configurations in an accurate, simple and reliable manner that can be used in research, clinical practice and training.
Introduction
Effective root canal treatment and endodontic surgery require a thorough knowledge of tooth anatomy and root canal morphology so that microorganisms and pulp tissue can be accessed and removed and root-ends managed properly (Cleghorn et al. 2008). In the human dentition, a wide range of anatomical variations in each tooth type has been reported in terms of the number and shape of roots and root canals (Vertucci 2005, Ahmed & Abbott 2012, Versiani et al. 2012, 2016, Ahmed 2013, Ahmed & Hashem 2016). For many decades, this topic has been the subject of numerous experimental and clinical reports, and it is clear that root and canal morphology vary greatly between populations, within populations and even within the same individual (Vertucci 2005, Ahmed & Cheung 2012, Ahmed 2015, Versiani et al. 2016).
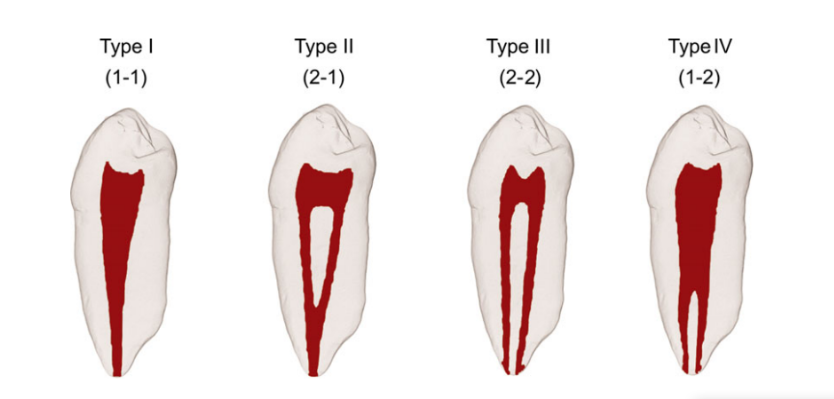
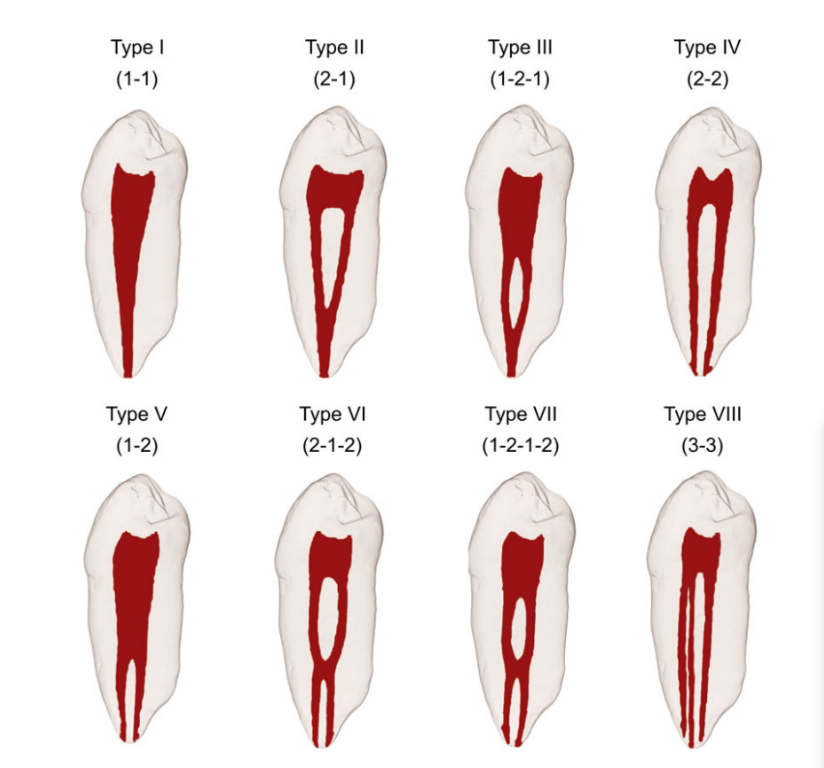
Data generated from the classical work of Hess & Zurcher (1925) to the more recent studies demonstrate that the ever-expanding knowledge on this subject required the creation of a classification system for defining root canal configuration. Using sectioning and radiographic methods, Weine et al. (1969) were the first to categorize root canal configurations within a single root into three types depending on the pattern of division of the main root canal along its course from the pulp chamber to the root apex (Fig. 1). Later, Vertucci et al. (1974) developed a classification system based on the evaluation of 200 cleared maxillary second premolars in which the pulp cavities were stained with dye; they found canal systems that were more complex than described by Weine and co-workers and identified a total of eight configurations (Fig. 2). Later, Weine (1982) added an additional type to his original system (Fig. 1).
Other classifications have also been introduced for specific tooth types, for example maxillary molars with four roots (Christie et al. 1991, Carlsen & Alexandersen 2000, Baratto-Filho et al. 2002, Versiani et al. 2012), maxillary premolars with three canals (Belizzi & Hartwell 1981, Ahmed & Cheung 2012), the middle mesial canal (Pomeranz et al. 1981) and distolingual root in mandibular molars (Song et al. 2010). More recently, Kottoor et al. (2012) and Albuquerque et al. (2012) suggested a new nomenclature to classify root canal anatomy in maxillary and mandibular molars, respectively.
Despite these efforts to systematically describe the diversity of canal configurations, additional types of root canal morphology have been reported by several authors within different populations (Gulabivala et al. 2001, 2002, Ng et al. 2001, Sert & Bayirli 2004, Versiani et al. 2016). Based on a review of previous reports on root canal morphology and results from recent anatomical studies using micro-CT technology, Versiani & Ordinola-Zapata (2015) described up to 37 root canal configuration types, which probably include the most common anatomical configurations that can be observed in a single root.
Notwithstanding these efforts, the creation of a simple classification system, able to be applied in all types of root and root canal configuration in all groups of teeth, has not been achieved.
Justification for a new classification system
The systems proposed by Weine et al. (1969), Vertucci et al. (1974) and Weine (1982) have been the most commonly used classifications and have been beneficial when categorizing many, but not all, canal config- urations. Recent reports on the identification of external and internal anatomical canal variations using advanced 3D imaging technology have revealed that the morphological characteristics of the root canal system are highly complex, and many canal configurations have been described as ‘nonclassifiable’ (Verma & Love 2011, Kim et al. 2013, Lee et al. 2014, Leoni et al. 2014). In fact, in one study, as many as 13% of specimens did not fit into the classification of Vertucci and co-workers (Filpo-Perez et al. 2015).
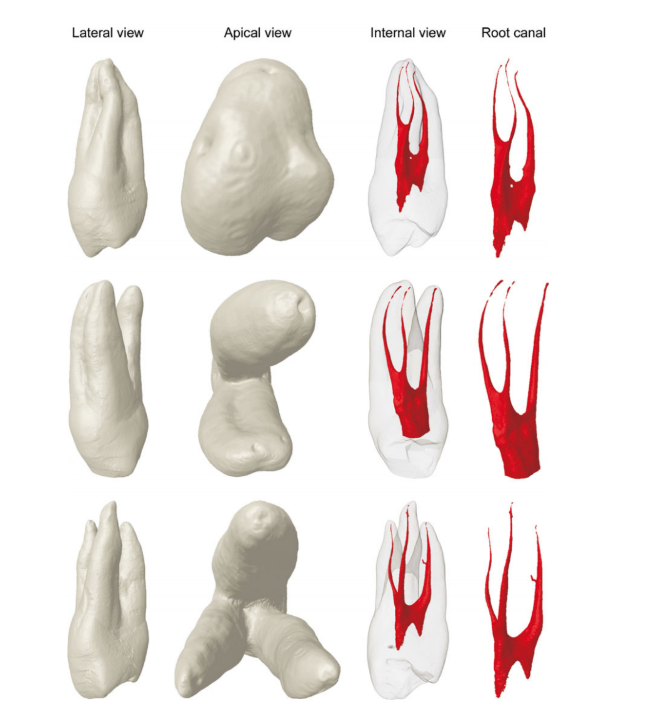
The literature also reveals inconsistencies regarding the classification of the internal anatomy of several tooth types, for example, maxillary premolar teeth with three canals, Vertucci et al. (1974) categorized this variation as type VIII and defined it as three separate, distinct root canals extending from the pulp chamber to the apex; however, no information is provided in the classification to describe whether these canals are encased in single-, double- or three-rooted teeth (Fig. 3). Therefore, in most of the studies, three- canalled single-/double-/three-rooted maxillary premolars continued to be referred to as type VIII configuration (Vertucci et al. 1974, Vertucci 1984, Velmurugan et al. 2005, Peiris 2008). Clearly, in terms of clinical management of teeth undergoing root canal treatment, it is critical to define the number of roots, and not just canals, as this will have implications in terms of access cavity preparation, mechanical instrumentation and root canal filling procedures (Ahmed & Cheung 2012).
Recently, Briseño-Marroquin et al. (2015) introduced a four-digit classification of root canal configurations, in which each root is divided into thirds (each third has a digit), with the fourth digit indicating the number of main foramina defined as the foramina that emerge from the same canal at the apical terminus and in which the measured diameter is no less than 0.2 mm. However, in this classification, there is no information on the configuration of the root component, and there are concerns on the practicality of using these criteria in the clinical situation, that is dividing the root into thirds, and defining the main apical foramina on the basis of their diameter.
New classification system for root and root canal morphology
Categorizing root canal configuration by ‘type’ using simple Roman numerals has been popular for more than 50 years. However, in recent years, a considerable volume of data has been generated on the morphological variations in root canals (Versiani & Ordinola-Zapata 2015), which has resulted in the systems used today for categorizing canal configurations into certain types based on a single number being insufficient and, indeed, inaccurate and misleading. The time has now come to develop a coding system that can be used to describe root and canal configurations that will aid clinicians, researchers and be of benefit to educators and students/trainees.
The new classification system suggested in this article aims to be simple, accurate and useful as it provides information on root and root canal anatomy. It does not address the degree of root and root canal curvature, degree of root/canal separation, the exact level of bifurcation of canals/roots, type of root fusion, accessory canals (lateral and furcation canals) nor apical deltas. Inclusion of these parameters was considered during the development of the proposed classification, but it became obvious that they added considerable complexity and the potential to lead to misunderstanding. Such additional information could be useful and in some ways provide a more accurate classification; however, the benefits of any new system must be simplicity so that it can be adopted universally.
The literature reveals many comprehensive classifications categorizing developmental anomalies related to the root or root canal such as dens invaginatus (Oehlers 1957), C-shaped canals (Melton et al. 1991, Fan et al. 2004, Kato et al. 2014), taurodontism (Shaw 1928, Jafarzadeh et al. 2008), supernumerary roots (Christie et al. 1991, Carlsen & Alexandersen 2000, Song et al. 2010), root fusions (Zhang et al. 2014) and others. For simplicity, the present classification will not reclassify abnormalities already addressed in the literature.
Aim
To create a simple, accurate and practical system that allows students/trainees, clinicians and researchers to classify root and root canal configurations identified using any diagnostic method regardless of their accuracy and reliability.
Objectives
- To describe the number of roots in all tooth types;
- To describe all known and yet-undiscovered root canal configurations.
Terminology
Root canal system
It is the space within the tooth that contains pulp tissue. The root canal system is divided into two portions: the pulp chamber, which is located in the anatomic crown of the tooth, and the root canal(s), encased in the root(s).
Root canal orifice
It is the opening of the canal system at the base of the chamber where the root canal begins. Generally, it is located at or just apical to the cervical line.
Root canal configuration
It is the course of the root canal system that begins at the orifice and ends at the canal terminus (minor apical diameter).
Major apical foramen
It is the exit of the root canal onto the external root surface, which is normally located within 3 mm of the root apex.
Minor apical foramen/apical constriction
It is the apical part of the root canal with the narrowest diameter which is generally 0.5–1.5 mm from the major apical foramen (Vertucci 2005). It is the reference point often used as the apical termination of canal instrumentation and filling procedures.
Classification
The new classification can be adapted for root and root canal configurations. It includes codes for three separate components: the tooth number, the number of roots, and the root canal configuration.
Tooth number
The tooth number (TN) can be written using any numbering system (e.g. universal numbering system, Palmer Notation Numbering System or the FDI World Dental Federation System). If the tooth cannot be identified using one of the numbering systems (i.e. extracted teeth), then a suitable abbreviation can be used, for example maxillary (upper) central incisor (UCI).
Number of roots and their configuration
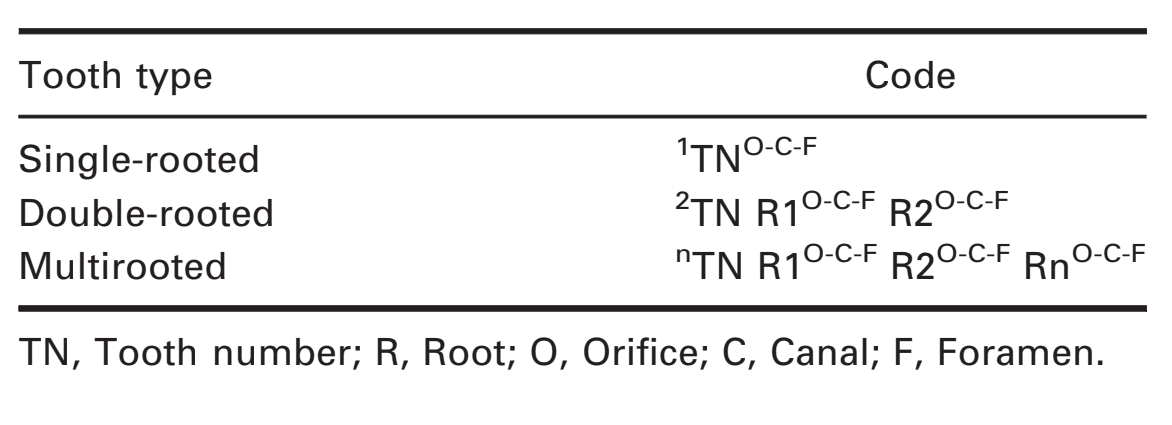
The number of roots (R) is added as a superscript before the tooth number (RTN). For instance, 1TN means that tooth ‘TN’ has one root. Any division of a root whether in the coronal, middle or apical third will be coded as two or more roots. Accordingly, a bifurcation is represented as 2TN, and trifurcation is represented as 3TN and so on. Details of roots in double- and multirooted teeth are added to the right of the tooth number (RTN Rn) (Table 1, Appendix S1).
Root canal configuration
The type of root canal configuration in each root will be identified as a superscript number(s) after the tooth number and will define the continuous course of the root canal system starting from the orifice(s) (O), through the canal (C) to the foramen (foramina) (F) (Table 1, Appendix S1).
Inevitably, the assessment of apical canal configurations may vary depending on the method used for identification – experimental or clinical, which can be rather subjective amongst different observers. For example, based on certain experimental measurements of canal dimensions or clinical negotiability, some apical bifurcations could either be classified as an apical delta/ramification (i.e. complex ramification of branches of the root canal located near, and open on, the root apex) or a division from the main canal (type 1-2). It is obvious that a standard consistent view of such anatomy cannot be achieved, and therefore, the apical canal configuration type should be classified based on the method and criteria used for identification.
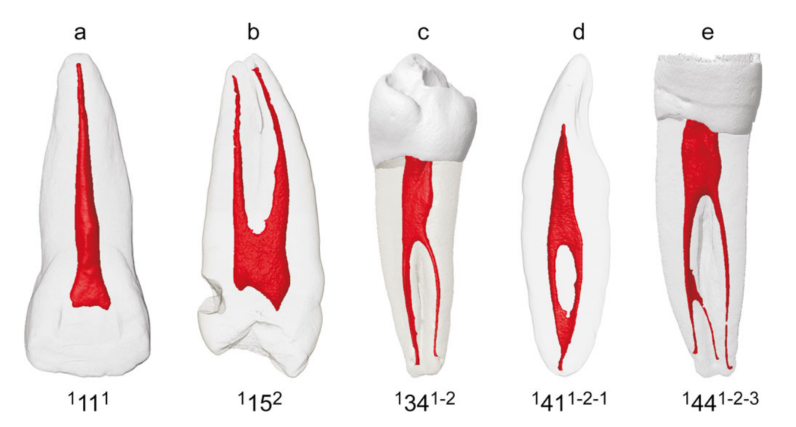
Single-rooted teeth
For any canal, if the numbers of O, C and F are the same, then a single code (1TNn) is used (Fig. 4). Thus, 1111 describes a single-rooted maxillary right central incisor having one orifice, one canal and one foramen (Fig. 4a), whilst 1152 describes a single-rooted maxillary right second premolar having two orifices, two independent canals and two foramina (Fig. 4b).
If the root has a varying number of O, C and/or F, then the configuration of the canal will be written to provide this detail (1TNO-C-F) (Fig. 4c,d). For instance, 1341-2 refers to a single-rooted mandibular left first premolar having one orifice and one canal initially but then bifurcating into two independent canals and having two apical foramina (Fig. 4c). 1411-2-1 refers to a single-rooted mandibular right central incisor having one orifice and one canal initially but then bifurcating into two independent canals and terminating in one canal (Fig. 4d), and 1441-2-3 refers to a single-rooted mandibular right first premolar having one orifice and one canal initially that bifurcates into two independent canals and terminates in three canals and three apical foramina (Fig. 4e).
Double-rooted teeth
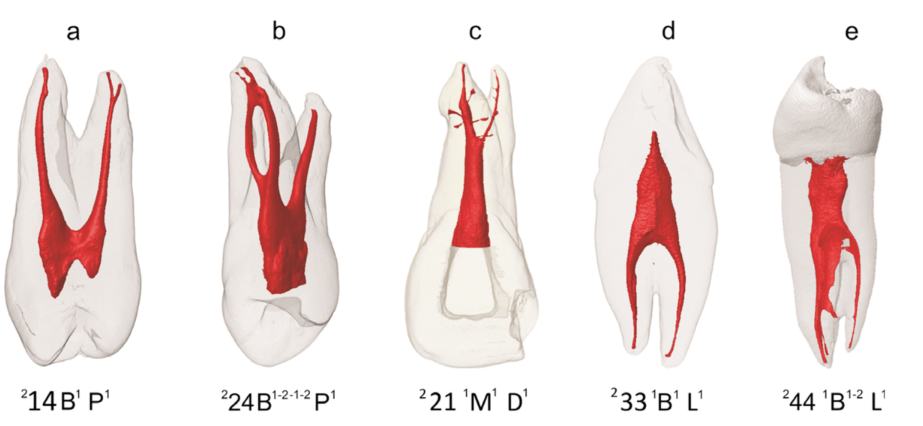
If a tooth is double-rooted, then the code 2TN R1O-C-F R2O-C-F should be used, where R1 and R2 describe the anatomy of the first and second roots, respectively (Fig. 5). As mentioned previously, only one code will be applied if the number of orifice(s), canal(s) and foramen (foramina) is the same, in the same root. For example, 214 B1 P1 refers to a double-rooted maxillary right first premolar in which each root (B: buccal; P: palatal) encases a single root canal from the orifice to the main foramen (Fig. 5a). 224 B1-2-1-2 P1 refers to a double-rooted maxillary left first premolar in which the buccal root encases a single canal leaving the chamber and dividing into two canals and then joining into one canal before dividing again into two separate canals until the canal terminus whilst the palatal root encases a single root canal from the orifice to the main foramen (Fig. 5b).
If the root bifurcates at the middle or apical third, and the root canal configuration is different apical and coronal to the level of root bifurcation, then the code will be 2TN O-CR1C-F R2C-F, where ‘O-C’ is the root canal configuration coronal to the level of bifurcation, and R1C-F R2C-F are the continuation of the canal and number of foramina apical to the level of the bifurcation in either first (R1) or second (R2) roots, respectively (Fig. 5c–e). Figure 5c shows a double-rooted maxillary left central incisor coded as 221 1M1 D1 in which the root bifurcates in the apical third and the root canal configuration apical and coronal the level of root bifurcation is different. Figure 5d,e shows similar anatomical variations of the root/root canal in a mandibular canine and premolar, respectively.
Multirooted teeth
If the tooth is multirooted, then the code nTN R1O-C-F R2O-C-F RnO-C-F should be used. As an example, 316 MB1 DB1 P1 means that the maxillary right first molar has three roots (MB: mesiobuccal; DB: distobuccal; P: palatal) and a single orifice, canal and foramen in each root (Fig. 6a). 316 MB2-1 DP1 P1 means that the maxillary right first molar has three roots in which the MB root encases canal type 2-1, whilst the DP and P roots encase a root canal with a single orifice, canal and foramen (Fig. 6b). Similarly, 417 MB2-1 DB1 MP1 DP1 means that the maxillary right second molar has four roots (MB: mesiobuccal; DB: distobuccal; MP: mesiopalatal; DP: distopalatal) in which the MB root encases canal type 2-1, and the DB, MP and DP roots encase a single orifice, canal and foramen in each root (Fig. 6c). 347 M2 DB1 DL1 means that the mandibular right second molar has three roots in which the mesial root (M) encases 2 independent canals, whilst the DB and DL (distolingual) roots encase a single root canal (Fig. 6d). Similar considerations will be applied if one of the roots bifurcates in the middle or apical third, and the root canal configuration is different apical and coronal the level of bifurcation.
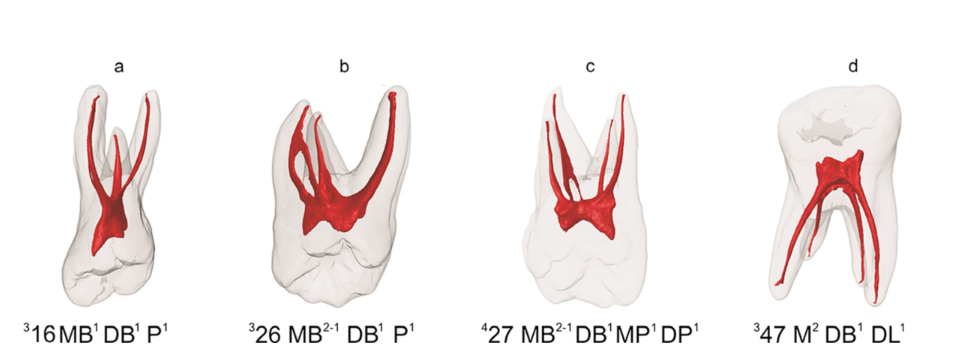
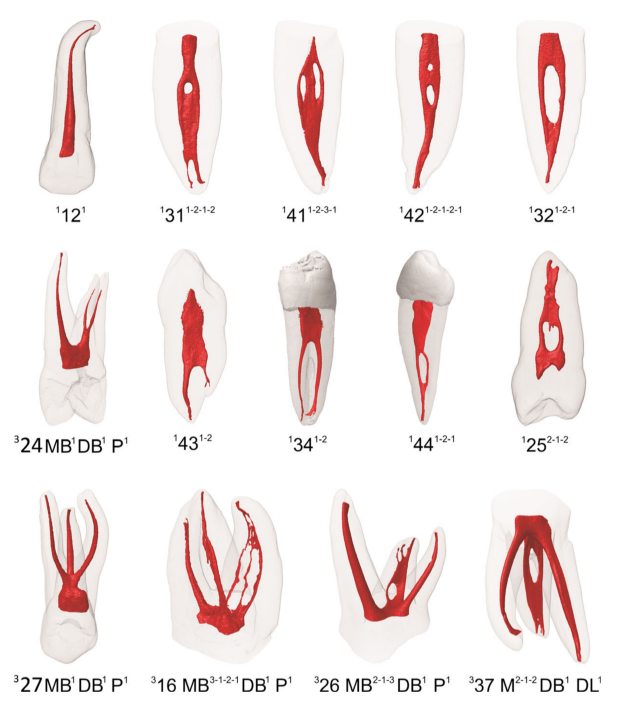
Figure 7 shows the application of the new configuration system on different types of root canal systems. Appendix S1 shows several examples of codes allocated for different teeth, root and root canal configuration types.
Conclusions
The new proposed classification attempts to provide a simple, accurate and practical system that allows students, dental practitioners and researchers to classify root and root canal configurations. It provides detailed information on the tooth number, number of roots and root canal configuration types, whilst excluding developmental anomalies and minor canal anatomy to pave the way for simplicity and universal adoption.
Authors: H. M. A. Ahmed, M. A. Versiani, G. De-Deus, P. M. H. Dummer
References:
- Ahmed HMA (2013) Anatomical challenges, electronic working length determination and current developments in root canal preparation of primary molar teeth. International Endodontic Journal 46, 1011–22.
- Ahmed HMA (2015) A paradigm evolution shift in the endodontic map. European Journal of General Dentistry 4, 98. Ahmed HMA, Abbott PV (2012) Accessory roots in maxillary molar teeth: a review and endodontic considerations. Australian Dental Journal 57, 123–31; quiz 248.
- Ahmed HMA, Cheung GSP (2012) Accessory roots and root canals in maxillary premolar teeth: a review of a critical endodontic challenge. ENDO - Endodontic Practice Today 6, 7–18.
- Ahmed HMA, Hashem AAR (2016) Accessory roots and root canals in human anterior teeth: a review and clinical considerations. International Endodontic Journal 48, 724–36.
- Albuquerque DV, Kottoor J, Velmurugan N (2012) A new anatomically based nomenclature for the roots and root canals-part 2: mandibular molars. International Journal of Dentistry 2012, 814789.
- Baratto-Filho F, Fariniuk LF, Ferreira EL, Pécora JD, Cruz-Filho AM, Sousa-Neto MD (2002) Clinical and macroscopic study of maxillary molars with two palatal roots. International Endodontic Journal 35, 796–801.
- Belizzi R, Hartwell G (1981) Evaluating the maxillary premolar with three canals for endodontic therapy. Journal of Endodontics 7, 521–7.
- Briseño-Marroquin B, Paqué F, Maier K, Willershausen B, Wolf TG (2015) Root canal morphology and configuration of 179 maxillary first molars by means of micro-computed tomography: an ex vivo study. Journal of Endodontics 41, 2008–13.
- Carlsen O, Alexandersen V (2000) Radix mesiolingualis and radix distolingualis in a collection of permanent maxillary molars. Acta Odontol Scandanvia 58, 229–36.
- Christie WH, Peikoff MD, Fogel HM (1991) Maxillary molars with two palatal roots: a retrospective clinical study. Journal of Endodontics 17, 80–4.
- Cleghorn BM, Goodacre CJ, Christie WH (2008) Morphology of teeth and their root canal systems. In: Ingle JI, Bakland LK, Baumgartner JC, eds. Ingle’s Endodontics, 6th edn. Hamilton: BC Decker Inc, pp 151–220.
- Fan B, Cheung GS, Fan M, Gutmann JL, Bian Z (2004) C- shaped canal system in mandibular second molars: part I- Anatomical features. Journal of Endodontics 30, 899–903.
- Filpo-Perez C, Bramante CM, Villas-Boas MH, Hungaro Duarte MA, Versiani MA, Ordinola-Zapata R (2015) Micro-computed tomographic analysis of the root canal morphology of the distal root of mandibular first molar. Journal of Endodontics 41, 231–6.
- Gulabivala K, Aung TH, Alavi A, Ng YL (2001) Root and canal morphology of Burmese mandibular molars. International Endodontic Journal 34, 359–70.
- Gulabivala K, Opasanon A, Ng YL, Alavi A (2002) Root and canal morphology of Thai mandibular molars. International Endodontic Journal 35, 56–62.
- Hess W, Zurcher E (1925) The anatomy of root canals of the teeth of the permenant and deciduous dentition. New York: William Wood.
- Jafarzadeh H, Azarpazhooh A, Mayhall JT (2008) Taurodontism: a review of the condition and endodontic treatment challenges. International Endodontic Journal 41, 375–88.
- Kato A, Ziegler A, Higuchi N, Nakata K, Nakamura H, Ohno N (2014) Aetiology, incidence and morphology of the C-shaped root canal system and its impact on clinical endodontics. International Endodontic Journal 47, 1012–33.
- Kim Y, Chang SW, Lee JK et al. (2013) A micro-computed tomography study of canal configuration of multiple-canalled mesiobuccal root of maxillary first molar. Clinical Oral Investigation 17, 1541–6.
- Kottoor J, Albuquerque DV, Velmurugan N (2012) A new anatomically based nomenclature for the roots and root canals-part 1: maxillary molars. International Journal of Dentistry 2012, 120565.
- Lee KW, Kim Y, Perinpanayagam H et al. (2014) Comparison of alternative image reformatting techniques in micro- computed tomography and tooth clearing for detailed canal morphology. Journal of Endodontics 40, 417–22.
- Leoni GB, Versiani MA, P´ecora JD, de Sousa-Neto MD (2014) Micro-computed tomographic analysis of the root canal morphology of mandibular incisors. Journal of Endodontics 40, 710–6.
- Melton DC, Krell KV, Fuller MW (1991) Anatomical and histological features of C-shaped canals in mandibular second molars. Journal of Endodontics 17, 384–8.
- Ng YL, Aung TH, Alavi A, Gulabivala K (2001) Root and canal morphology of Burmese maxillary molars. International Endodontic Journal 34, 620–30.
- Oehlers FA (1957) Dens invaginatus (dilated composite odontome). I. Variations of the invagination process and associated anterior crown forms. Oral Surgery Oral Medicine Oral Pathology 10, 1204–18.
- Peiris R (2008) Root and canal morphology of human permanent teeth in a Sri Lankan and Japanese population. Anthropological Science 116, 123–33.
- Pomeranz HH, Eidelman DL, Goldberg MG (1981) Treatment considerations of the middle mesial canal of mandibular first and second molars. Journal of Endodontics 7, 565–8.
- Sert S, Bayirli GS (2004) Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. Journal of Endodontics 30, 391–8.
- Shaw JC (1928) Taurodont teeth in South African races. Journal of Anatomy 62, 476–98.
- Song JS, Choi HJ, Jung IY, Jung HS, Kim SO (2010) The prevalence and morphologic classification of distolingual roots in the mandibular molars in a Korean population. Journal of Endodontics 36, 653–7.
- Velmurugan N, Parameswaran A, Kandaswamy D, Smitha A, Vijayalakshmi D, Sowmya N (2005) Maxillary second premolar with three roots and three separate root canals– case reports. Australian Endodontic Journal 31, 73–5.
- Verma P, Love RM (2011) A Micro CT study of the mesiobuccal root canal morphology of the maxillary first molar tooth. International Endodontic Journal 44, 210–7.
- Versiani MA, Ordinola-Zapata R (2015) Root canal anatomy: implications in biofilm disinfection. In: Chavez de Paz L, Sedgley C, Kishen A (Org.) (eds). Root canal biofilms, 1st edn. Toronto: Springer, 2014, Vol. 1, pp. 23–52.
- Versiani MA, Pécora JD, de Sousa-Neto MD (2012) Root and root canal morphology of four-rooted maxillary second molars: a micro-computed tomography study. Journal of Endodontics 38, 977–82.
- Versiani MA, Ordinola-Zapata R, Kele s A et al. (2016) Middle mesial canals in mandibular first molars: a micro-CT study in different populations. Archives of Oral Biology 61, 130–7.
- Vertucci FJ (1984) Root canal anatomy of the human permanent teeth. Oral Surgery, Oral Medicine and Oral Pathology 58, 589–99.
- Vertucci FJ (2005) Root canal morphology and its relationship to endodontic procedures. Endodontic Topics 10, 3–29. Vertucci F, Seelig A, Gillis R (1974) Root canal morphology of the human maxillary second premolar. Oral Surgery,
- Oral Medicine and Oral Pathology 38, 456–64. Weine FS (1982) Endodontic therapy, 3rd edn. St. Louis: Mosby.
- Weine FS, Healey HJ, Gerstein H, Evanson L (1969) Canal configuration in the mesiobuccal root of the maxillary first molar and its endodontic significance. Oral Surgery, Oral Medicine and Oral Pathology 28, 419–25.
- Zhang Q, Chen H, Fan B, Fan W, Gutmann JL (2014) Root and root canal morphology in maxillary second molar with fused root from a native Chinese population. Journal of Endodontics 40, 871–5.