Worldwide Prevalence of a Lingual Canal in Mandibular Premolars: A Multicenter Cross-sectional Study with Meta-analysis
Abstract
Introduction: The presence of multiple root canals is an important morphologic aspect of mandibular premolars. This study aimed to perform a worldwide analysis on the prevalence of a lingual canal in mandibular premolars and to evaluate its influence on patients’ demographics in 23 countries using cone-beam computed tomographic images.
Methods: Observers from 23 countries were instructed to evaluate cone-beam computed tomographic images of 300 first and 300 second premolars (13,800 teeth) regarding the presence of a lingual canal, canal configuration, and data related to patients’ ethnicity, age, and sex following a standardized screening methodology. Intra- and interrater evaluations were performed using the Cohen kappa test and intraclass correlation coefficient. Proportion and odds ratio forest plots were calculated in order to compare groups. Statistical significance was set at 5%.
Results: Both kappa and intraclass correlation coefficient values were above 0.60, and the percentage of agreement was 94.9% (first premolar) and 97.8% (second premolar). A significant statistical difference was observed between the worldwide proportion of a lingual canal in mandibular first (23.8%; range, 12.0%–32.7%) and second (5.3%; range, 1.0%–15.3%) premolars (P ˂ .05). Asians and patients over 60 years old were associated with the lowest proportions of a lingual canal (P ˂ .05), whereas Africans and younger groups were associated with the highest proportions (P ˂ .05). The prevalence of a lingual canal in males (27.9%) was higher than females (20.0%) for the first premolar only (P ˂ .05). Males were associated with 1.533 and 1.597 higher odds of presenting a lingual root canal in the first and second premolars, respectively.
Conclusions: The worldwide proportion of a lingual root canal was 23.6% and 5.3% for the first and second premolars, respectively. Ethnicity, geographic region, age, and sex had an influence on the outcomes. (J Endod 2021;■:1–12.)
In mandibular premolars, several morphologic variations of the root and root canals have been reported in the literature including the presence of radicular grooves, C-shaped configuration, furcation canals, apical ramification, 3-rooted morphology, and double canals. Double canals are usually classified as a Vertucci type V configuration and refer to the presence of a second root canal positioned on the lingual side; they are more likely to be noticed in first premolars. The orifice of the lingual canal usually has a sharp entry angle and is located at the middle (69%) or apical (31%) thirds, which may contribute to it going unnoticed clinically. The relatively high prevalence of this additional canal in mandibular premolars is possibly 1 of the most relevant anatomic features in this group of teeth considering that missed or untreated root canals appeared to have an adverse effect on endodontic outcomes. In the last decade, the root canal configuration of mandibular premolars has been addressed not only in laboratory studies using high-resolution micro–computed tomographic technology but also through in vivo prevalence studies using cone-beam computed tomographic (CBCT) imaging. A recent systematic review using CBCT assessment found 7 studies from 6 countries reporting the prevalence of the lingual canal in the mandibular first premolar and 5 studies from 4 countries on the second premolar. Although additional data from different populations were published after this review, the worldwide prevalence and impact of the lingual canal in mandibular premolars remain unknown in most geographic regions. Moreover, there are no studies evaluating its influence on demographic factors, such as sex, age, or ethnicity, as reported with other anatomic features. Therefore, the aim of the present study was to perform an in vivo worldwide analysis regarding the prevalence of a lingual root canal in mandibular premolars and its relationship to patient demographics (ethnicity, age, and sex) using CBCT images. The null hypotheses tested were that there were no differences in the prevalence of the lingual canal in mandibular premolars considering
- geographic regions,
- ethnicity,
- age, and
- sex.
Materials and methods
Research Protocol and Sample Size Calculation
This study followed a previous publication that described the preferred reporting items for epidemiologic cross-sectional studies on root and root canal anatomy using CBCT technology and received the previous approval of an ethics committee. The presence of a lingual root canal (the primary outcome) and the canal configuration (the secondary outcome) of mandibular first and second premolars was assessed by 23 specialists in endodontics from 23 different geographic regions using preexisting CBCT images.
Before the analysis, all observers were provided simultaneously with written guidelines containing a detailed description of the assessment methodology, a tutorial video explaining step-by-step the screening process of the CBCT data sets for both primary and secondary outcomes, bibliographic references, and group deadlines. The sample size for this study was calculated based on the results of a previous publication that compared 2 specific geographic region groups and used similar methodology. For the primary outcome, considering a power of 80% and an alpha-type error of 0.05, the final sample sizes for the mandibular first and second premolars were 287 (effect size of 8.9) and 233 (effect size of 4.3), respectively. In order to counterbalance that no sample size calculation was performed for the comparison of the other geographic regions, the number of teeth per group was increased to 300.
Sample Selection and Data Acquisition
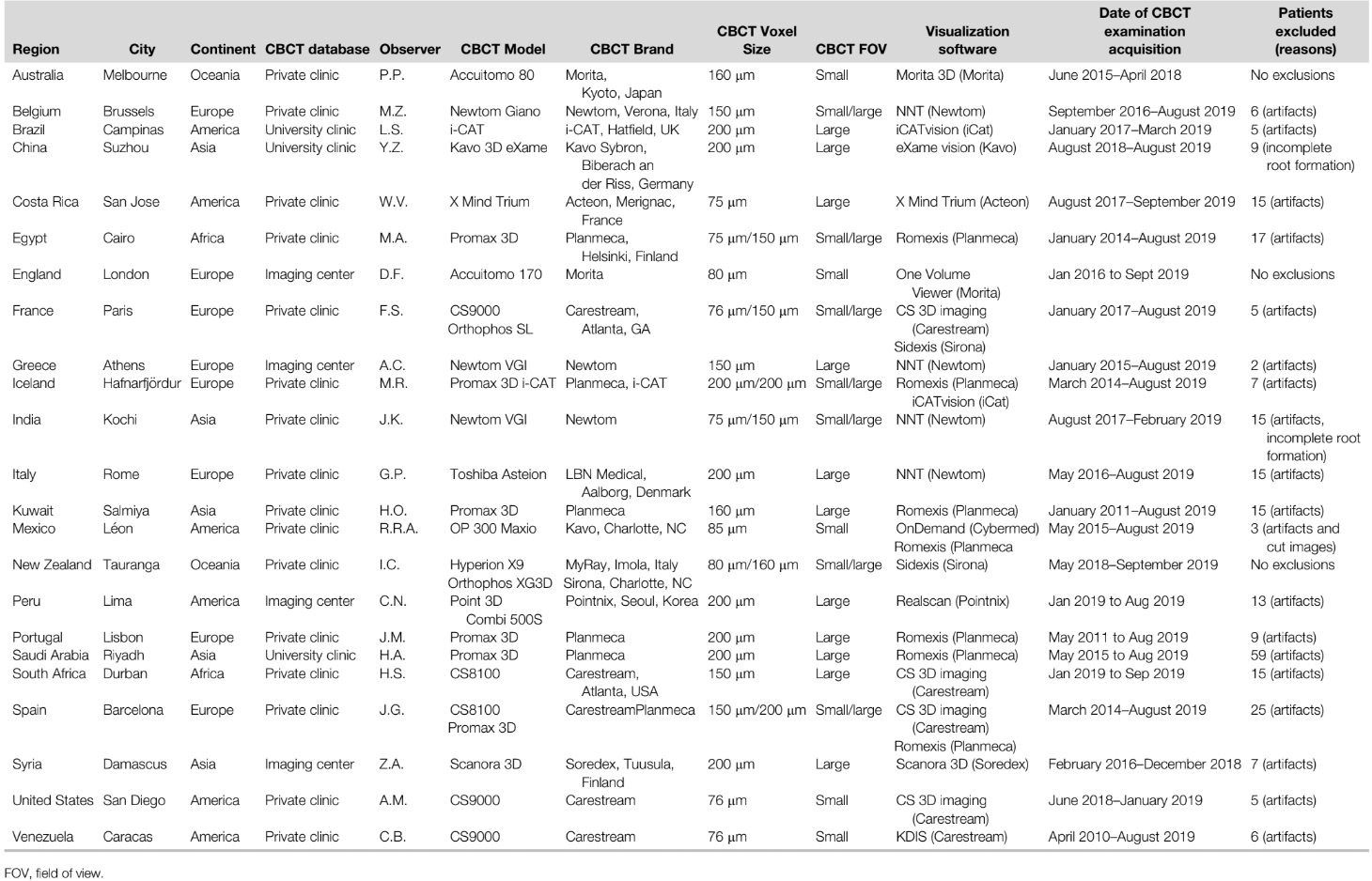
The population in this study included a convenience sample made up of patients attending private practices from 23 different geographic regions. Demographic (ethnicity, age, and sex) and quantitative data were acquired by assessing preexisting CBCT databases containing at least 1 mandibular premolar. CBCT data sets were reviewed consecutively according to their numeric or alphabetic chart order until the sample size for each tooth group (n = 300) was reached. Any type of CBCT scanner or field of view was acceptable as long as the voxel size was equal or less than 200 μm; more than 1 scanner was allowed in each region if the assessment was conducted by the same observer (Table 1). The exclusion criteria were as follows: teeth with previous root canal treatment, root resorption, or incomplete root formation; uncertainty regarding tooth numbering; absence of demographic information; or visualization compromised by imaging artifacts.
CBCT Imaging Assessment
To evaluate the CBCT images, the axial, coronal, and sagittal planes of each premolar root were aligned to the vertical and horizontal marking lines of the software. Then, each premolar was classified according to its type (first or second premolar), the number of roots (apical split was not considered a multirooted configuration), and the presence of a lingual canal (primary outcome). Additionally, as a secondary outcome, each tooth was classified as having a single canal, 2 independent canals (from the pulp chamber to the apex), 2 confluent canals (2 separate canals leaving the chamber but merging to form a single canal at the apex), or more than 2 canals. For these analyses, observers were allowed to change some visualization settings, such as filters or noise reduction, to improve imaging assessment. In case of doubt, they were asked to consult the main researcher (J.M.) to reach a consensus. All data were recorded in a standard Excel (Microsoft, Redmond, WA) sheet and further screened by the main researcher for nonconformities. Observers were blinded to the other outcomes to avoid any influence bias on their results.
Observer Reliability
Intra- and interrater evaluations were performed before the assessment of the selected CBCT databases. The intrarater reliability was assessed between 2 subsequent repeated records (1-month interval) taken by the observers (first and second evaluations) on the analysis of 10% of randomly selected teeth (n = 30 premolars) regarding the presence of a lingual canal (primary outcome) acquired from their own CBCT databases. The Cohen kappa test was used to measure the reliability of each observer. For interrater analysis, all observers evaluated the same 10 CBCT large field of view data sets (not included in the final analysis) containing 18 mandibular premolars from each group (n = 36) regarding the presence of a lingual canal according to the data assessment protocol during the same time window. The interrater reliability was measured by both the intraclass correlation coefficient (ICC) and the percentage of agreement. Additionally, these results obtained from each observer were compared with a consensus classification reached by 2 experienced external evaluators using the Cohen kappa test. If the ICC and kappa values were below 0.60 for the primary outcome in the intra- and/or interrater evaluations, the observer was asked to review the research protocol and to repeat the evaluation.
Statistical Analysis
Considering the multicenter nature of the present study, a meta-analysis was conducted based on a random effects model16. Data were analyzed using OpenMeta[Analyst] v. 10.10 software (http://www.cebm.brown.edu/openmeta/), and the results for the primary outcome (the presence of a lingual canal) were presented as forest plots displaying the odds ratio and untransformed proportions with a 95% confidence interval (CI). Meta-regression was used to understand the possible sources of heterogeneity. Statistical significance was set at P ˂ .05.
Results
Supplemental Table S1 (available online at www.jendodon.com) shows that all intra- and interrater kappa values were above 0.60, whereas the ICC and percentage of agreement values were 0.988 and 94.9% (first premolar) and 0.991 and 97.8% (second premolar).
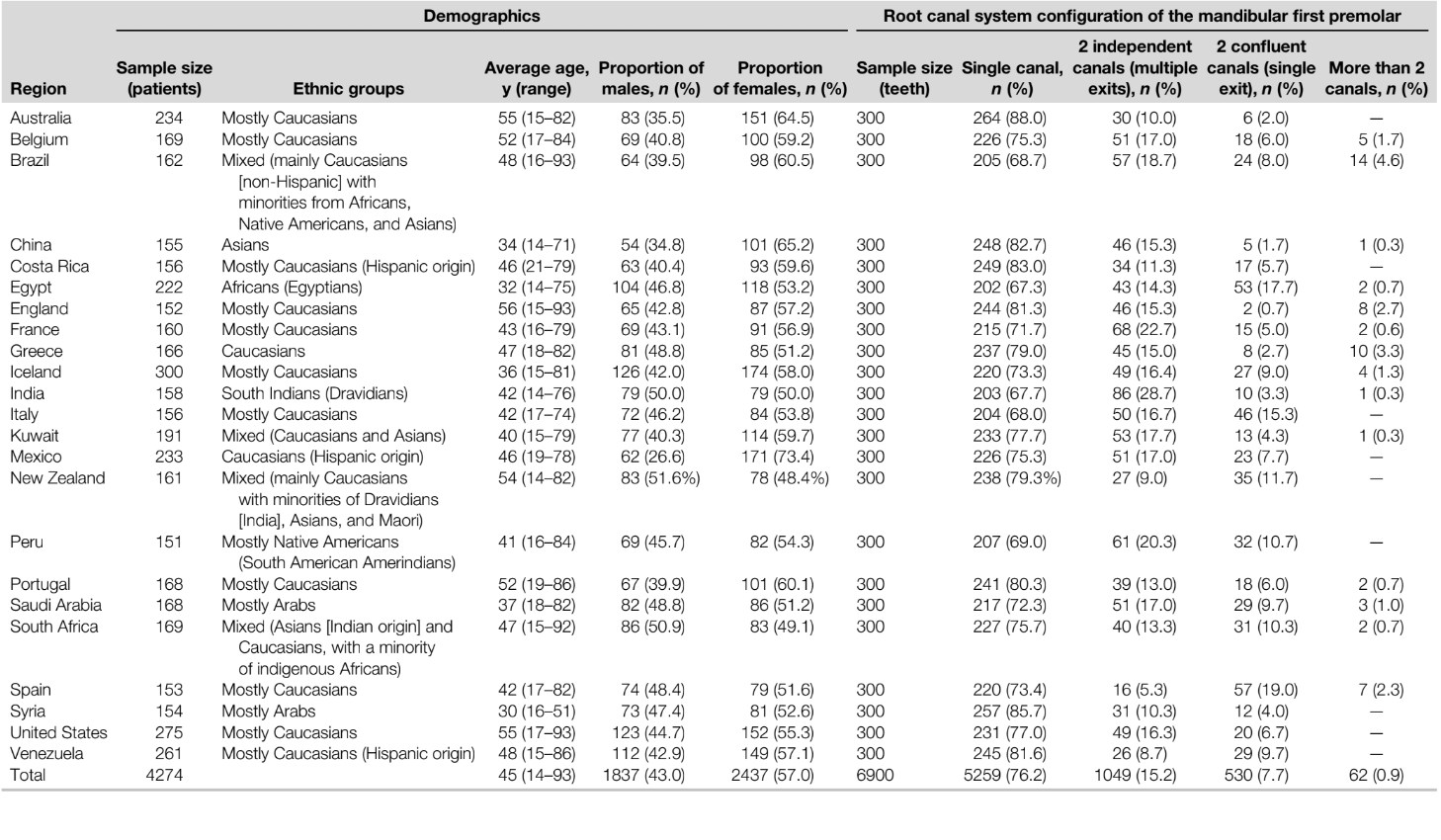
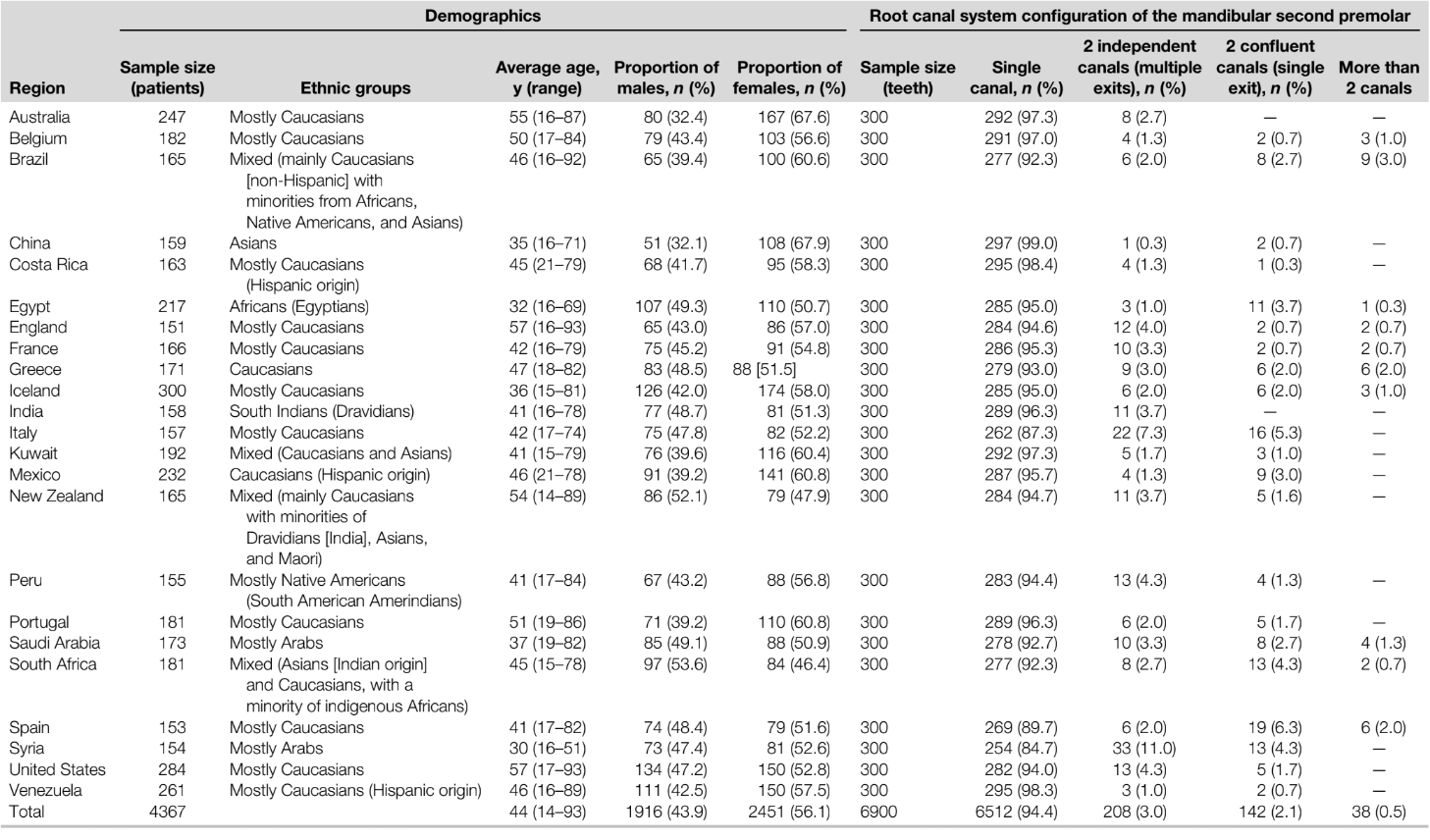
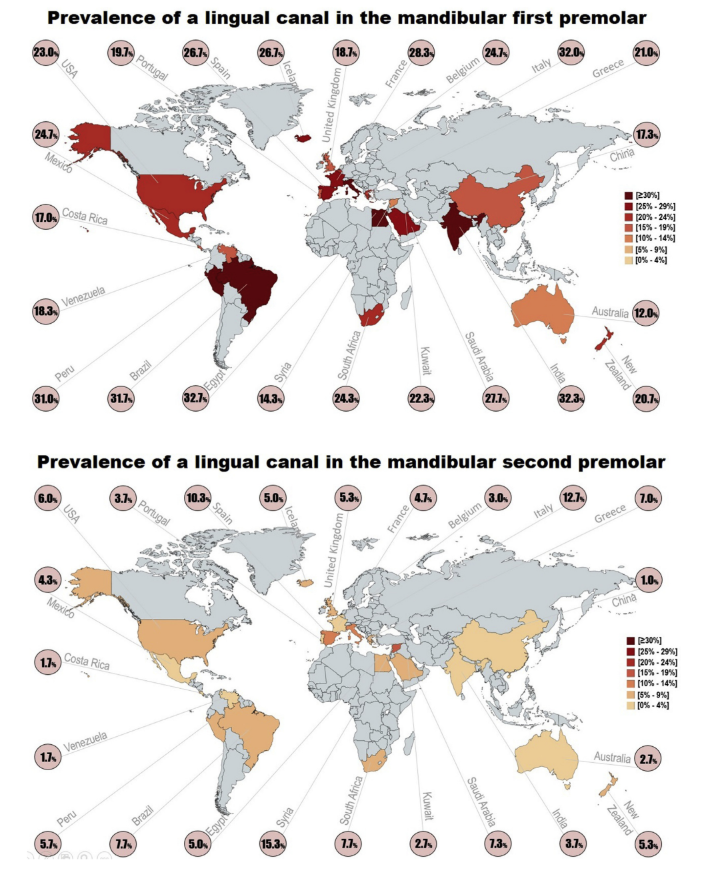
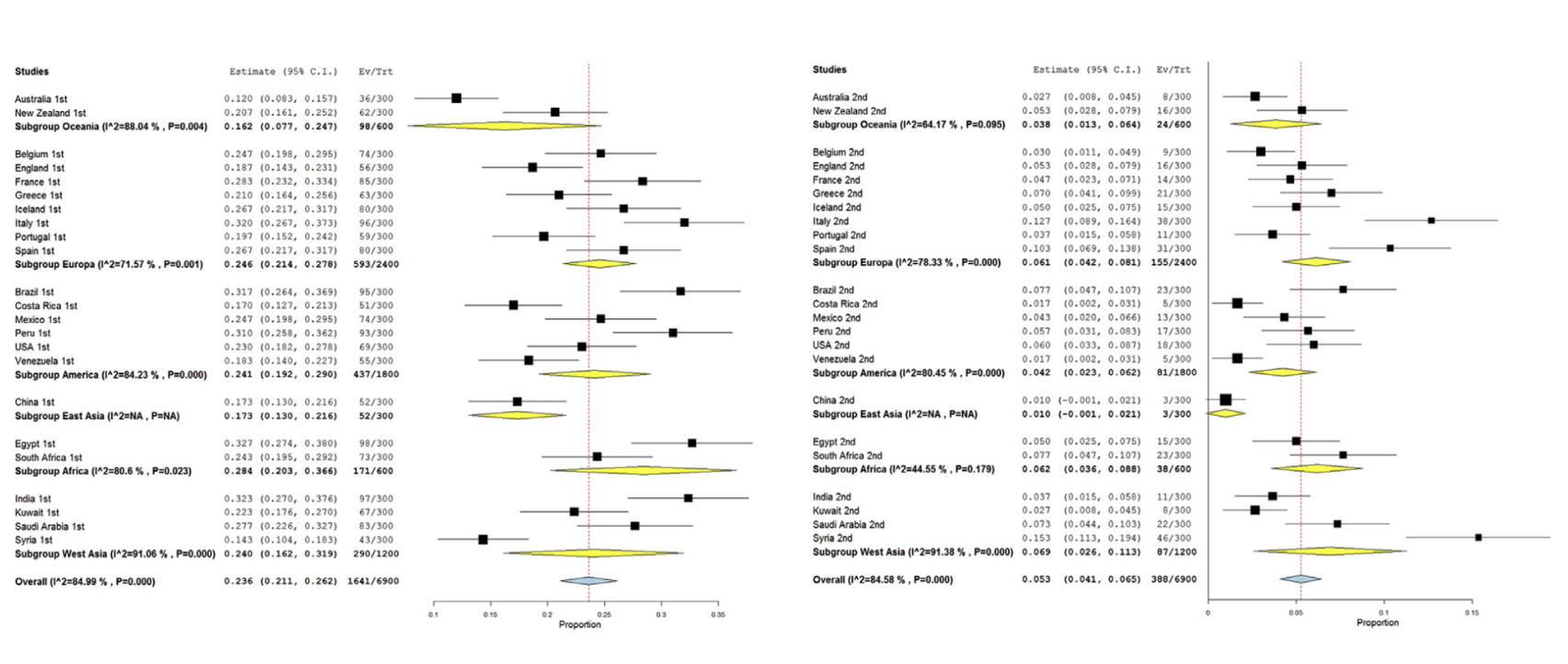
Imaging voxel size meta-regression showed an almost constant proportion of a lingual root canal when comparing results using different voxel sizes (between 75 and 200 μm) for both premolars (Supplemental Fig. S1 is available online at www.jendodon.com). Considering the omnibus P values for the first (0.224) and second (0.091) premolars, the heterogeneity of the results could not be explained by the image voxel size. Tables 2 and 3 summarize the demographic characteristics of the patients and the root canal configuration of 13,800 mandibular premolars (6900 teeth from each group) from more than 4270 patients. Overall, the worldwide proportion of a lingual canal in the mandibular premolar was 23.8% (95% CI, 21.1%–26.2%), varying from 12.0% (95% CI, 8.3%–15.7% [Australia]) to 32.7% (95% CI, 27.4%–38.0% [Egypt]), whereas a global percentage of 5.3% (95% CI, 4.1%–6.5%) was observed in the second premolars with proportions ranging from 1.0% (95% CI, 0.0%–2.1% [China]) to 15.3% (95% CI, 11.3%–19.4% [Syria]) (Fig. 1; Supplemental Fig. S2 is available online at www.jendodon.com). The difference in the worldwide proportion of lingual canals observed in the first and second premolar teeth was considered statistically significant (P ˂ .05; Supplemental Fig. S2 is available online at www.jendodon.com).
Data analysis from geographic regions showed that Oceania (16.2% [95% CI, 7.7%–24.7%]) and East Asia (17.3% [95% CI, 13.0%–21.6%]) had the lowest proportions of lingual canals in mandibular first premolars, whereas the highest was observed in Africa (28.4% [95% CI, 20.3%–36.6%]); however, no differences were noted among regions (P ˃ .05, Fig. 2). For the second premolar, the differences were significant (P ˂ .05), with the lowest proportions found in East Asia (1.0% [95% CI, 0.0%–2.1%]) and Oceania (3.8% [95% CI, 1.3%–6.4%]) and the highest percentages (˃6%) in Europe, Africa, and West Asia (Fig. 2). Regarding ethnicity, some mixed groups (Brazil, Kuwait, New Zealand, and South Africa) were excluded from the analysis because of their ethnic diversity.
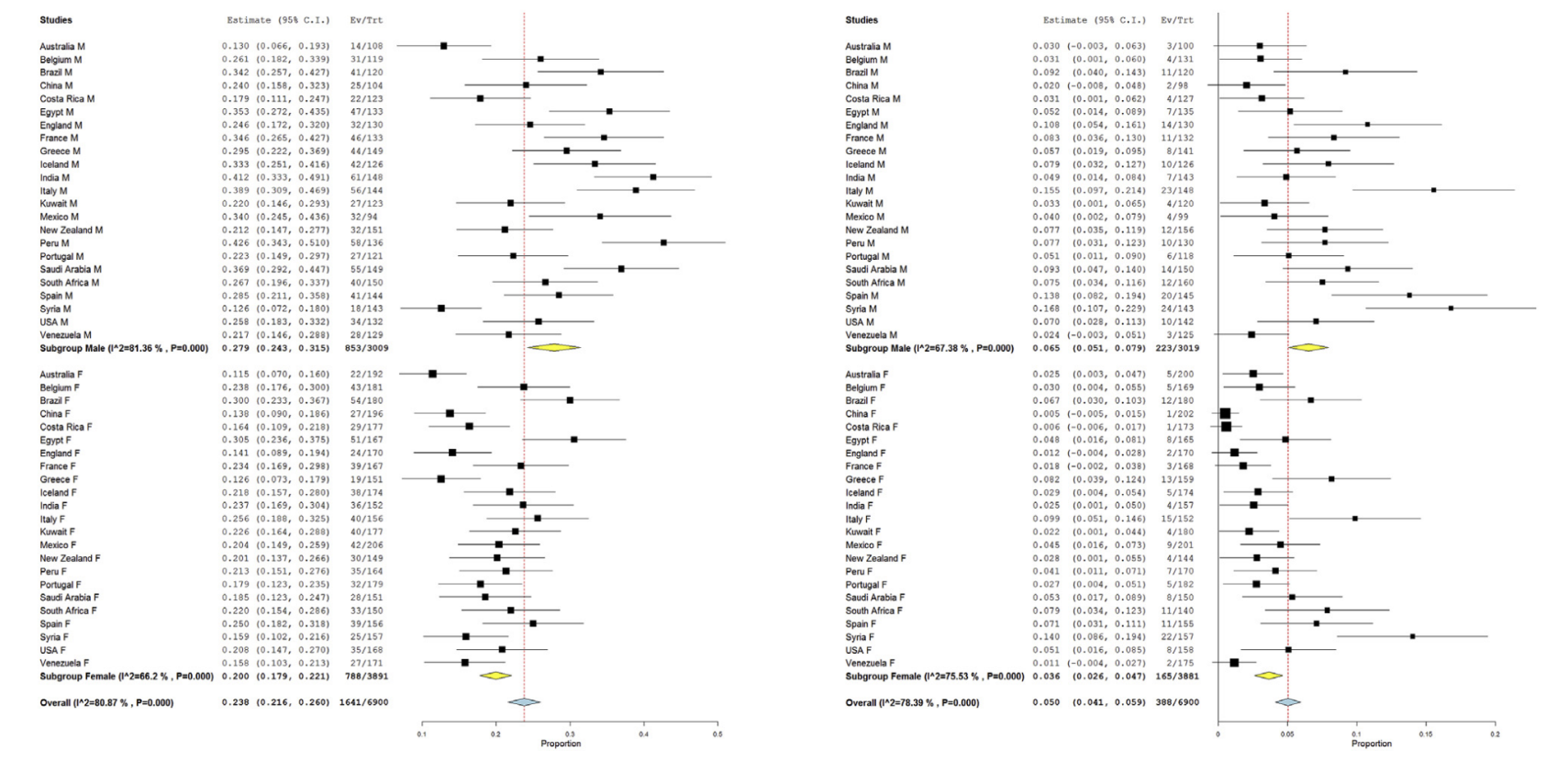
Asians showed the lowest proportions of a lingual canal for both groups of teeth compared with the other ethnic groups (P ˂ .05, Fig. 3). Older patients (˃60 years old) also presented lower proportions compared with younger groups, but a statistical significance was only reached for the first premolar (P ˂ .05; Supplemental Fig. S3 is available online at www.jendodon.com). In male patients, the prevalence of a lingual canal in the first premolars was 27.9% (95% CI, 24.3%– 31.5%), whereas in females it was 20.0% (95% CI, 17.9%–22.1%; Fig. 4). The proportion difference between sexes was considered statistically significant for both premolars (P ˂ .05, Fig. 4). Moreover, males were associated with significantly higher odds of presenting a lingual canal in both first (1.533 [95% CI, 1.329–1.768]) and second (1.597 [95% CI, 1.287–1.982]) premolars (P ˂ .05; Supplemental Fig. S4 is available online at www.jendodon.com).

Discussion
In the present study, an in vivo worldwide analysis was performed to evaluate the prevalence of a lingual root canal in mandibular premolars and its relationship to patient demographics by assessing preexisting CBCT databases; thus, no patient was exposed to radiation for the purpose of this research. The multicenter nature of this study and the analytical tool used to access the root and root canal morphologies (CBCT imaging) allowed the evaluation of a large number of teeth (N = 13,800 teeth) that could be distributed into subgroups according to their demographic characteristics while maintaining a high statistical power. This methodological design also enabled exploration of this anatomic variation throughout the world (23 countries), including several geographic regions not assessed in any previous in vivo study with a low voxel size (Australia, Belgium, Costa Rica, France, Egypt, Greece, Iceland, India, Kuwait, Mexico, New Zealand, Peru, Saudi Arabia, South Africa, Spain, Syria, United Kingdom, United States, and Venezuela), providing new findings with high external validity. Overall, the mean worldwide prevalence of a lingual canal in the mandibular first premolar was 23.6% (Supplemental Fig. S2 is available online at www.jendodon.com), a percentage quite similar to the ones reported in previous studies in different countries such as Brazil (19.1%), Italy (20.8%), South Korea (21.2%), Portugal (22.2%), Taiwan (26.6%), and Turkey (28.6%). It should be noted that previous studies on Chinese patients consistently reported lower percentages of this additional anatomy in mandibular premolars (13.2%, 13.4%, and 18.9%) than the average, which is also in line with the outcome of the present investigation (17.3%). On the other hand, some regional analysis did not corroborate with the literature, and high percentages were noted (Brazil: 31.7% and Italy: 32.0%; Fig. 1). Similarly, a higher prevalence of multiple canals in mandibular first premolars was also reported in the German population (78.1%). However, authors considered apical ramifications as part of the main root canal system, which partially explains this dissimilarity. Regarding the mandibular second premolars, the mean worldwide prevalence of a lingual root canal was 5.3% (Supplemental Fig. S2 is available online at www.jendodon.com), a significantly lower percentage when compared with first premolars but in agreement with previous investigations. Again, the results of mandibular second premolars from Asian patients were under the average (1.0%) (Fig. 1), confirming previous research in the Chinese population (0.4% and 2.8%).
In relation to patient demographics, analysis of the results showed significant differences (Figs. 2–4 and Supplemental Fig. S3 is available online at www.jendodon.com); therefore, the null hypotheses were rejected. Geographic location and ethnicity (Figs. 2and 3) are closely related factors, and their understanding pushes us back to the origin of human species and the early colonization of the world. Modern anthropological studies indicate that the human origins may be in Kenya in the African continent. From there, the early humans moved north through the Levant corridor or east through the Horn of Africa, giving origin to the 3 main ethnic groups: Africans, Caucasians (northern Eurasian expansion), and Asian (eastern Asian expansion). This early human migration led to several differences observed among Caucasians, Africans, and Asians because their evolutions were made independently from each other for thousands of years during world colonization. Their genome became an evolutionary result of genetic heritability and environmental influences such as dietary modification. As a result, it is likely that differences in the mandibular premolar phenotype, based on geographic region or ethnicity, may have existed for a long time.
Traditionally, anthropological studies focus on crown or external root morphology traits and landmarks and not on root canal configuration. Comparative research evaluating anatomic landmarks of the mandibular premolar crowns concluded that some primitive hominid traits were preserved in Homo erectus located in the suburban area of Beijing when compared with their ancestors, with divergences also being observed in comparison to European Pleistocene ancestral populations. Overall, it has been stated that Africans are among the ones presenting the largest teeth, whereas Asians and Europeans have similar sizes. Considering the reported influence of the external morphology on the internal root canal anatomy, it has been proposed that the highest proportion of multiple canals in Africans and the lowest percentages on Asians may be related to teeth size, reflecting the evolutionary process of these 2 ethnic groups. For instance, the lowest proportion of multiple canals in the mandibular premolars of Asian populations observed in the present study not only corroborates with previously published data but is also consistent with results reported to other tooth groups, such as the second canal in the mesiobuccal root of maxillary molars and the lingual canal in mandibular anterior teeth.
The root canal space can be understood as a dynamic system that changes over time due to pathologic or physiological events. In the present study, older patients (˃ 60 years old) were associated with the lowest presence of a lingual canal in the first premolar (19.1%) (Supplemental Fig. S3 is available online at www.jendodon.com), possibly as a consequence of physiological deposition of secondary dentin. This narrowing process may reduce the root canal system to sizes that may become undetectable even through high-resolution CBCT imaging. However, the present results are not in agreement with 2 previous findings that reported no difference in the prevalence of additional canals in mandibular premolars due to aging. However, it is important to note that the sample size in these studies comprised only a small number of mandibular first premolars (n = 97 and n = 154, respectively), resulting in a reduced statistical power compared with our sample size (N = 6900). Considering the analysis of sex, the low prevalence of multiple canals in 1 root observed in the female group in both mandibular premolars (Fig. 4 and Supplemental Fig. S4 is available online at www.jendodon.com) corroborates the results reported for other tooth groups such as maxillary molars and mandibular central incisors. In fact, the percentage difference between males and females regarding the prevalence of a lingual canal in the mandibular first premolar (~8%) is not only statistically significant but also clinically relevant. Sexual dimorphism is well recognized in dental sciences. For instance, forensics use metric and nonmetric dental measurements to perform sex estimation. Previous research in several populations reported males as having larger tooth sizes compared with females,a characteristic that may be related to the influence of the X and Y chromosomes on growth, in which Y promotes crown dentin and enamel formation and X seems to limit enamel grow. These morphologic differences may help to partially explain the lowest number of additional canals in the female group.
The root canal system of mandibular premolars has been addressed using several in vivo and ex vivo methodological approaches using different analytical tools. Nowadays, micro–computed tomographic technology is considered the gold standard to evaluate root canal morphology. However, considering it is a laboratory tool, it is impractical and quite expensive to evaluate the influence of certain anatomic components on demographic factors using large-sized groups. This is 1 of the main advantages of using non-destructive CBCT imaging because it allows the analysis of a large volume of data by assessing preexisting databases. On the other hand, the most relevant limitation of CBCT imaging is related to its limited spatial resolution, which has been considered inappropriate in identifying fine anatomic features. In the present study, both primary and secondary outcomes were obtained by means of CBCT images and consisted in the analysis of the main root canal system configuration only, avoiding the assessment of smaller anatomic structures, such as lateral canals or apical deltas.
Additionally, the main canal morphology was investigated in CBCT data sets from different centers using voxel sizes between 75 and 200 μm. This could be interpreted as a potential confounding factor, but this variable was excluded as a major source of bias in accordance with other meta-regression studies.
One important limitation of multicenter studies is the difficulty to guarantee that all observers perform the data assessment using a standardized methodological approach.
Aiming to minimize this potential bias, observers were chosen based on their large experience in the endodontic field, and the primary outcome was reduced to a dichotomous response (the presence/ absence of a lingual root canal). In addition, intra- and interrater reliability measurements were conducted to guarantee trustworthy results. Consequently, the methodological standardization for imaging assessment was validated in all centers of the 23 countries, allowing the meta-analysis statistical comparisons in order to explore possible heterogeneities and confounders, as previously done in similar studies.
Notwithstanding, as in any other cross- sectional study, the present evaluation was based on only 1 point in time. This may lead to some limitations when performing the interpretation of age results (eg, because factors not related to physiological aging, such as pathologic dentin deposition due to caries, restorative procedures, or periodontal problems, were not possible to be assessed).
Further studies should continue exploring other geographic regions in order to collect more data with clinical and anthropological interest in order to analyze the influence of demographic factors on the root canal morphology.
Conclusions
The mean prevalence of a lingual root canal in the mandibular first premolar (23.6%) was significantly higher than in the mandibular second premolar (5.3%). Demographic characteristics influenced the final outcomes. Asian ethnicity and older patients (˃ 60 years old) had the lowest prevalence of lingual canals in mandibular premolars, whereas the highest proportions and odds were observed in males for both teeth.
Authors: Jorge N. R. Martins, Yuerong Zhang, Murilo von Zuben, Walter Vargas, Hussein C. Seedat, Fabio Santiago, Ruben Rosas Aguilar, Magnus F. Ragnarsson, Gianluca Plotino, Peter Parashos, Hani F. Ounsi, Christian Nole, Adam Monroe, Jojo Kottoor, Jose Antonio Gonzalez, Daniel Flynn, Antonis Chaniotis, Imran Cassim, Carlos Boveda, Luiza Berti, Zaher Altaki, Moataz-Bellah A. M. Alkhawas, Hussam Alfawaz, Emmanuel J. N. L. Silva and Marco Aurelio Versiani
References:
- Fan B, Ye W, Xie E, et al. Three-dimensional morphological analysis of C-shaped canals in mandibular first premolars in a Chinese population. Int Endod J 2012;45:1035–41.
- Ordinola-Zapata R, Bramante CM, Villas-Boas MH, et al. Morphologic micro-computed tomography analysis of mandibular premolars with three root canals. J Endod 2013;39:1130–5.
- Liu N, Li X, Liu N, et al. A micro-computed tomography study of the root canal morphology of the mandibular first premolar in a population from southwestern China. Clin Oral Investig 2013;17:999–1007.
- Boschetti E, Silva-Sousa YT, Mazzi-Chaves JF, et al. Micro-CT evaluation of root and canal morphology of mandibular first premolars with radicular grooves. Braz Den J 2017;28:597–603.
- Li X, Liu N, Liu N, et al. A micro-computed tomography study of the location and curvature of the lingual canal in the mandibular first premolar with two canals originating from a single canal. J Endod 2012;38:309–12.
- Karabucak B, Bunes A, Chehoud C, et al. Prevalence of apical periodontitis in endodontically treated premolars and molars with untreated canal: a cone-beam computed tomography study. J Endod 2016;42:538–41.
- Burklein S, Heck R, Schafer E. Evaluation of the root canal anatomy of maxillary and mandibular premolars in a selected German population using cone-beam computed tomographic data. J Endod 2017;43:1448–52.
- Martins JNR, Marques D, Silva E, et al. Prevalence studies on root canal anatomy using cone- beam computed tomographic imaging: a systematic review. J Endod 2019;45:372–86.
- Yu X, Guo B, Li KZ, et al. Cone-beam computed tomography study of root and canal morphology of mandibular premolars in a western Chinese population. BMC Med Imaging 2012;12:18.
- Corbella S, Baruffaldi M, Perondi I, Taschieri S. Cone-beam computed tomography investigation of the anatomy of permanent mandibular premolars in a cohort of Caucasians. J Investig Clin Dent 2019;10:e12373.
- Jang YE, Kim Y, Kim B, et al. Frequency of non-single canals in mandibular premolars and correlations with other anatomical variants: an in vivo cone beam computed tomography study. BMC Oral Health 2019;19:272.
- Wu D, Hu DQ, Xin BC, et al. Root canal morphology of maxillary and mandibular first premolars analyzed using cone-beam computed tomography in a Shandong Chinese population. Medicine (Baltimore) 2020;99:e20116.
- Martins JN, Marques D, Silva E, et al. Prevalence of C-shaped canal morphology using cone beam computed tomography - a systematic review with meta-analysis. Int Endod J 2019;52:1556–72.
- Martins JN, Kishen A, Marques D, et al. Preferred reporting items for epidemiologic cross- sectional studies on root and root canal anatomy using cone-beam computed tomographic technology: a systematized assessment. J Endod 2020;46:915–35.
- Martins JN, Gu Y, Marques D, et al. Differences on the root and root canal morphologies between Asian and White ethnic groups analyzed by cone-beam computed tomography. J Endod 2018;44:1096–104.
- Basagana X, Pedersen M, Barrera-Gomez J, et al. Analysis of multicentre epidemiological studies: contrasting fixed or random effects modelling and meta-analysis. Int J Epidemiol 2018;47:1343–54.
- Caputo BV. Estudo da Tomografia Computadorizada de Feixe Co^nico na Avaliaça~o Morfolo´gica de raizes e canais dos molares e pre´ molares da populaça~o brasileira (PhD thesis). Sa~o Paulo: Universidade de Sa~o Paulo; 2014.
- Martins JNR, Francisco H, Ordinola-Zapata R. Prevalence of C-shaped configurations in the mandibular first and second premolars: a cone-beam computed tomographic in vivo study. J Endod 2017;43:890–5.
- Wu YC, Su CC, Tsai YC, et al. Complicated root canal configuration of mandibular first premolars is correlated with the presence of the distolingual root in mandibular first molars: a cone-beam computed tomographic study in Taiwanese individuals. J Endod 2017;43:1064–71.
- Arslan H, Capar ID, Ertas ET, et al. A cone-beam computed tomographic study of root canal systems in mandibular premolars in a Turkish population: theoretical model for determining orifice shape. Eur J Dent 2015;9:11–9.
- Hanihara T. Geographic structure of dental variation in the major human populations of the world. In: Scott R, Irish J, editors. Anthropological Perspectives on Tooth Morphology. Genetics, Evolution, Variation. 1st ed. New York: Cambridge University Press; 2013. p. 479–509.
- Yaacob H, Nambiar P, Naidu MD. Racial characteristics of human teeth with special emphasis on the Mongoloid dentition. Malays J Pathol 1996;18:1–7.
- Potter RH, Yu PL, Dahlberg AA, et al. Genetic studies of tooth size factors in Pima Indian families. Am J Hum Genet 1968;20:89–100.
- Irish J. Afridonty: the “Sub-Saharan African Dental Complex” revisited. In: Scott GR, Irish J, editors. Anthropological Perspectives on Tooth Morphology. Genetics, Evolution, Variation. 1st ed. New York: Cambridge University Press; 2013. p. 278–95.
- Xing S, Zhou M, Liu W. Crown morphology and variation of the lower premolars of Zhoukoudian Homo erectus. Chinese Sci Bull 2009;54:3905–15.
- 26. Mizoguchi Y. Significant among-population associations found between dental characters and envirinmental factors. In: Scott R, Irish J, editors. Anthropological Perspectives on Tooth Morphology. Genetics, Evolution, Variation. 1st ed. New York, NY: Cambridge University Press; 2013. p. 108–25.
- Martins JNR, Marques D, Joao E, et al. Second mesiobuccal root canal in maxillary molars-a systematic review and meta-analysis of prevalence studies using cone beam computed tomography. Arch Oral Biol 2020;113. 104589.
- Martins JNR, Marques D, Leal Silva EJ, et al. Influence of demographic factors on the prevalence of a second root canal in mandibular anterior teeth - a systematic review and meta-analysis of cross-sectional studies using cone beam computed tomography. Arch Oral Biol 2020;116. 104749.
- Johnstone M, Parashos P. Endodontics and the ageing patient. Aust Dent J 2015;60:20–7.
- Thomas RP, Moule AJ, Bryant R. Root canal morphology of maxillary permanent first molar teeth at various ages. Int Endod J 1993;26:257–67.
- Capitaneanu C, Willems G, Thevissen P. A systematic review of odontological sex estimation methods. J Forensic Odontostomatol 2017;2:1–19.
- Lakhanpal M, Gupta N, Rao N, Vashisth S. Tooth dimension variations as a gender determinant in permanent maxillary teeth. JSM Dent 2013;1:1014–9.
- Alvesalo L. The expression of human sex chromossome genes in oral and craniofacial growth. In: Scott GR, Irish J, editors. Anthropological Perspectives on Tooth Morphology. Genetics, Evolution, Variation. 1st ed. New York: Cambridge University Press; 2013. p. 92–107.
- Sousa TO, Hassan B, Mirmohammadi H, et al. Feasibility of cone-beam computed tomography in detecting lateral canals before and after root canal treatment: an ex vivo study. J Endod 2017;43:1014–7.
- Cesaroni G, Forastiere F, Stafoggia M, et al. Long term exposure to ambient air pollution and incidence of acute coronary events: prospective cohort study and meta-analysis in 11 European cohorts from the ESCAPE Project. BMJ 2014;348:f7412.