
Influence of access cavity preparation on the dentine thickness of mesial canals of mandibular molars prepared with reciprocating instruments
Abstract
Aim: To evaluate the influence of traditional and conservative access cavity preparations on the remaining dentine thickness in the coronal third of mesial canals of extracted mandibular molars prepared with reciprocating instruments using micro-computed tomography as the analytical tool.
Methodology: Seventy extracted mandibular molars were scanned at a pixel size of 19 μm. From this initial sample, 20 teeth were selected, pair-matched and distributed into two groups (n = 10) according to the access cavity preparation: traditional (TradAC) or conservative (ConsAC). The root canals were sequentially enlarged with Reciproc Blue R25 (size 25, 0.08v taper) and R40 (size 40, 0.06v taper) instruments. A new scan was performed and the postoperative stacks were coregistered with their respective preoperative datasets. A colour-coded cross sections of the roots were created and used to identify and measure the smallest dentine thickness related to both MB and ML canals at 1.0-mm intervals from the furcation level of up to 5 mm in the apical direction, in both mesial and distal aspects of the roots, before and after preparation. The statistical analyses were performed with paired-samples t-test, independent-samples Student T-test and Chi-Square test with a significance level of 5%.
Results: At all levels of both groups, dentine thickness before preparation was greater than after preparation (p < .05). No difference in the percentage of dentine reduction was observed between TradAC and ConsAC groups (p > .05), but a significantly greater reduction was observed to the distal aspect of the roots (p < .05). After root canal preparation, dentine thinner than 0.5 mm was observed mostly along the distal aspect of the root (10% to 15%) of the MB and ML canals, with no influence of the access cavity type on its incidence to either mesial (X2 = 1.66; p = .2) or distal (X2 = 0.40; p = .5) directions. In the TradAC group, dentine thickness in most slices was greater than 1.0 mm after preparation (n = 124) whilst, in the ConsAC, it ranged from 0.5 to 1.0 mm (n = 136).
Conclusion: Traditional or conservative access cavity preparation in extracted mandibular molars did not influence the remaining dentine thickness in the coronal third of mesial canals enlarged with thermomechanically treated nickel–titanium reciprocating instruments.
Introduction
Minimally invasive endodontics was founded on preserving hard tooth tissues during root canal treatment aiming to maintain optimal strength, fracture resistance and several other characteristics needed for the long-term function and survival of root filled teeth (Clark & Khademi, 2010a, 2010b). Based on this concept, several access cavity preparation types were proposed to preserve the maximum tooth structure, including the pulp chamber roof and pericervical dentine (Clark & Khademi, 2010a, 2010b; Neelakantan et al., 2018; Silva et al., 2020a). Whilst in the traditional access cavity preparation (TradAC) the roof of the pulp chamber is completely removed to obtain straight-line access to the canal orifices (Ingle, 1985; Patel & Rhodes, 2007), the conservative access cavity (ConsAC) was designed to maintain as much of the pulp chamber roof as possible. Even though this topic has emerged as a trend in endodontic research and this procedure has been adopted by several clinicians, its influence on the fracture resistance of teeth has only limited supporting evidence since most of the studies demonstrated no difference when comparing teeth prepared with traditional or conservative access cavities (Silva et al., 2020a). Although it would be desirable to preserve tooth structures during root canal treatment, it has been reported that ConsAC might leave anatomical interferences that can compromise proper canal shaping, cleaning and disinfection procedures (Alovisi et al., 2018; Barbosa et al., 2020; Pedullà et al., 2018; Silva et al., 2020a, 2020b; Vieira et al., 2020).
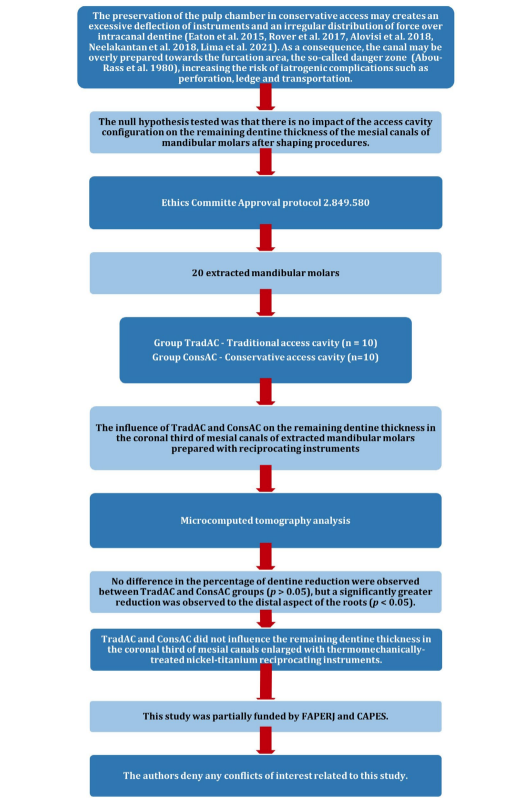
In mandibular molars, a conservative access may impair the quality of canal shaping procedures because the preservation of the pulp chamber roof creates an excessive deflection of instruments and an irregular distribution of force over intracanal dentine (Alovisi et al., 2018; Eaton et al., 2015; Lima et al., 2021; Neelakantan et al., 2018; Rover et al., 2017). As a consequence, the canal may be overly prepared towards the furcation area, the so-called danger zone (Abou-Rass et al., 1980), increasing the risk of iatrogenic complications such as perforation, ledge and transportation. The danger zone in the mesial root of mandibular molars has been extensively studied with reported values of minimum dentine thickness ranging from 0.78 to 1.1 mm at the furcation area (Garcia Filho et al., 2003; Kessler et al., 1983; Lim & Stock, 1987; Montgomery, 1985). This is an important aspect mostly because, recently, De-Deus et al. (2019) revisited the danger zone concept and observed that the thinnest dentine surrounding mesial canals of mandibular molars also occurred towards the mesial portion of the root in 40% of the evaluated cross-sectional slices.
In the literature, however, no publications focusing on the evaluation of the influence of conservative access cavities on the remaining dentine thickness after root canal preparation have been identified. Thereby, the aim of this study was to evaluate the influence of the access cavity preparation on remaining dentine thickness along the coronal third of mesial canals of extracted mandibular molars after canal preparation with reciprocating instruments, using micro-CT technology as the analytical tool. The null hypothesis tested was that there is no impact of the access cavity configuration on remaining dentine thickness of the mesial canals of mandibular molars after shaping procedures.
Material and methods
The manuscript of this laboratory study has been written according to Preferred Reporting Items for Laboratory studies in Endodontology 2021 guidelines (Nagendrababu et al., 2021). Figure 1 is a visual representation of the study design and its outcomes.
Sample size calculation
The effect size for this study (2.62) was based on the data from a previous study (Keleş et al., 2020). The analysis was performed using two independent means from the T-test family in G*Power 3.1 software (Henrick Heine-Universität) with α = 0.05 and 95% power inputs. Ten specimens (five per group) were considered the ideal sample size to observe significant difference between groups. Five samples were added to each group (n = 10) to increase reliability and compensate possible sample loss during the experimental procedures.
Sample selection, imaging and groups
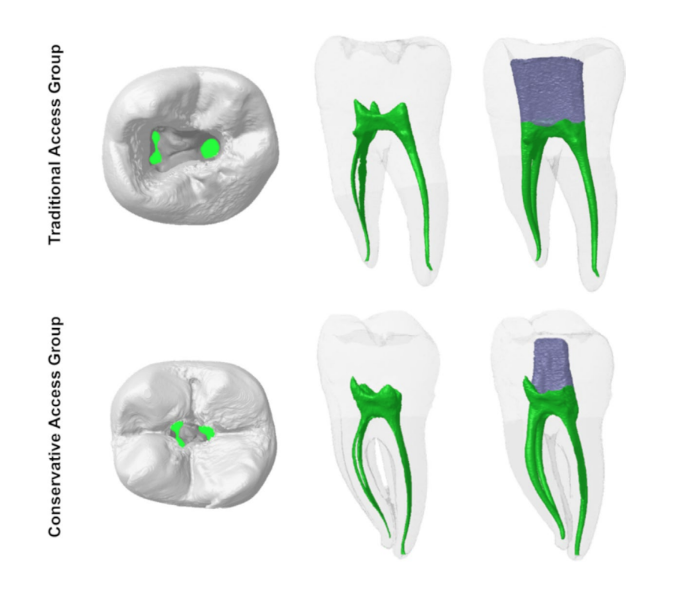
After local ethics committee approval (protocol 2.849.580), 70 mandibular molars were extracted and stored in distilled water for no longer than 6 months. All teeth had similar length and root curvature less than 20° (Schneider 1971), but no restoration, deep caries, fracture or incomplete root formation. Teeth were scanned at a pixel size of 19 μm in a micro-CT device (SkyScan 1174v.2, Bruker-microCT) set at 50 kV, 800 mA, 180° rotation with steps of 0.5° and frame averaging of 2. X-rays were filtered through a 0.5-mm-thick aluminium filter. Images were reconstructed (NRecon v. 1.7.4.2; Bruker-microCT) using standardized parameters of beam hardening (40%), ring artefact (7) and smoothing (5), resulting in the acquisition of 800 to 900 transaxial cross sections per tooth. Three-dimensional models of the root canals were created using CTAn v.1.18.8 (Bruker-microCT) and evaluated regarding configuration, length, volume and geometry (structure model index). Then, 20 molars with mesial roots having Vertucci's Type II or Type IV canal configurations were selected, anatomically matched and allocated into two groups (n = 10), according to the access cavity preparation type: traditional or conservative (Figure 2).
Before the experimental procedures, each tooth was mounted on a mannequin in a phantom head to simulate clinical conditions. Then, a specialist in endodontics with 5 years of clinical experience performed all access cavities and canal preparations. Procedures were performed under operating microscope magnification (×16) and high illumination (DF Vasconcelos, Valença).
Access cavity preparation
Traditional access cavity (TradAC) was performed with 1014HL (KG Sorensen) and Endo Z (Dentsply Sirona) burs. The pulp chamber roof was removed completely to obtain straight access to the canal orifices, as previously described (Ingle, 1985; Patel & Rhodes, 2007). ConsAC were prepared with 1014HL and 3080 burs (KG Sorensen) starting at the central fossa and extending up to the point where the canal orifices could be located using a size 08 K-file (Dentsply Sirona), partially preserving the pulp chamber roof (Clark & Khademi, 2010b).
Root canal preparation
Root canals were initially negotiated with a size 08 K-file (Dentsply Sirona). Then, after confirming apical patency with a size 10 K-file (Dentsply Sirona), a glide path was performed with a size 15 K-file (Dentsply Sirona) up to the working length, established 1 mm from the apical foramen. Root canals were sequentially enlarged up to the working length with Reciproc Blue R25 (size 25, 0.08v taper) and R40 (size 40, 0.06v taper) instruments (VDW) mounted on a VDW Silver motor (VDW) set at RECIPROC ALL motion, using three cycles of in-and-out movements with slight apical pressure and amplitude of 3 mm. After each cycle, the instrument was removed from the canal and cleaned with sterile gauze. In each canal, a total of 10 mL of 2.5% sodium hypochlorite (NaOCl) was delivered 3 mm short of the working length with a 30G Navitip needle (Ultradent) adapted to a 5-mL plastic syringe. Final irrigation was performed using 2 mL of 2.5% NaOCl (1 min), followed by 2 mL of 17% EDTA (1 min) and 2 mL of distilled water. One instrument was used to prepare the root canal system of each mesial root and discarded.
Micro-CT analysis
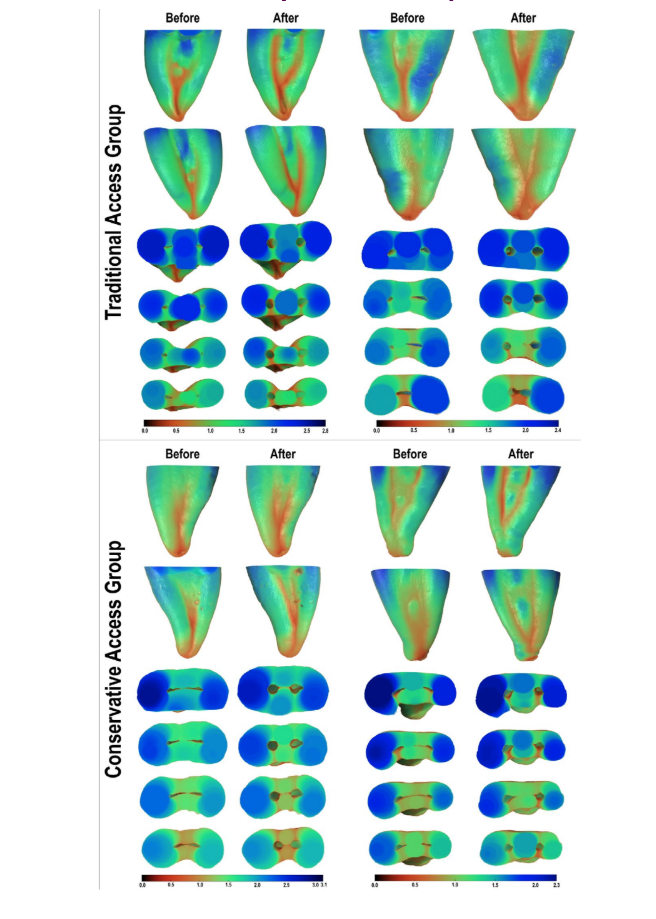
After chemomechanical preparation, a new scan and reconstruction were performed using the previously mentioned parameters. Then, the postoperative stacks were coregistered with their respective preoperative datasets using the affine algorithm of the 3D Slicer v.4.3.1 software (available at http://www.slicer.org). The region of interest was selected extending from the furcation level up to 5 mm towards the apical direction. An image analysis routine was established to measure the minimal dentine thickness at 1.0-mm intervals using the Fiji/Image J software (Fiji), in a total of 120 transaxial slices per group. Initially, a median filter of three was applied and the dentine was binarized with the intermode threshold. Then, the BoneJ plugin (Doube et al., 2010) was applied to create colour-coded cross sections of the roots and to measure the smallest dentine thickness related to the mesiobuccal (MB) and mesiolingual (ML) canals, before and after preparation, in both mesial and distal aspects of the roots. Then, dentine thickness values were categorized as <0.5, 0.5–1.0 and >1.0 mm, and their percentage frequencies calculated. Using CTAn v.1.18.8 software (Bruker-microCT), a 3D mapping of the dentine thickness (before and after preparation procedures) was created, saved for structure thickness and qualitatively compared using 3D colour-coded models of the matched roots with CTVox v.3.3.0 software (Bruker-microCT).
Statistical analysis
Normal distribution of data was confirmed (Shapiro–Wilk test, p > .05). Paired-samples t-test and independent-samples Student's t-test were used to compare the dentine thickness within and between TradAC and ConsAC groups respectively. The percentage frequencies of cross-sectional slices with dentine thickness less than 0.5 mm after preparation were compared between groups using a Chi-square test. BioStat software (v. 5.0.1 AnalystSoft) was used to perform the statistical analysis with a significance level set at 5%.
Results
Tables 1 and 2 show the descriptive statistics (mean, standard deviation and range values) of dentine thickness measured at each level, before and after preparation of MB and ML canals, at both mesial and distal positions of teeth prepared with TradAC and ConsAC, whilst Figure 3 depicts colour-coded 3D models of representative mesial roots.
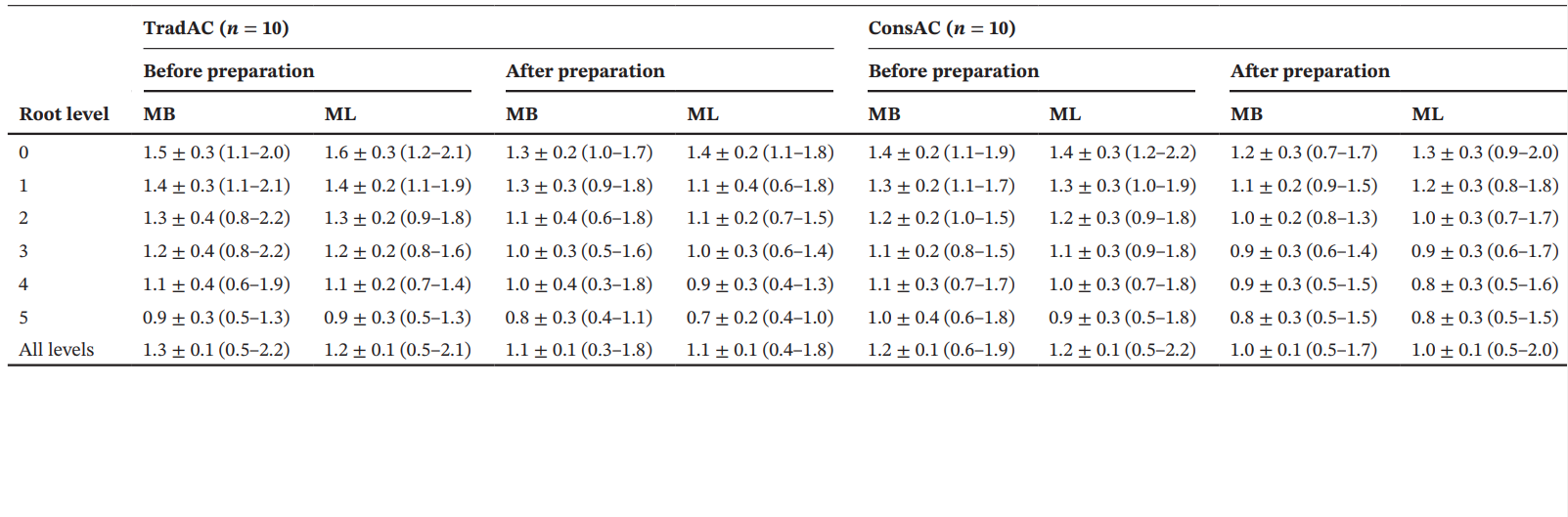
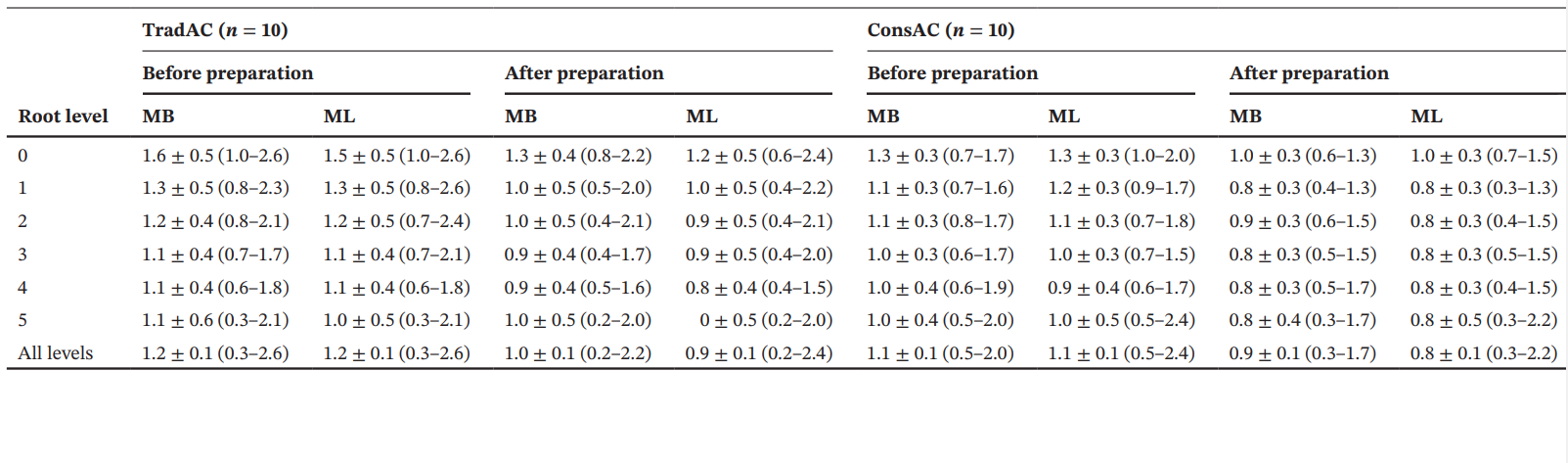
In all levels of both groups, dentine thickness before preparation was greater than after preparation (p < .05). The analysis of the percentage reduction in dentine thickness revealed no significant difference between TradAC and ConsAC groups for both MB and ML canals (p > .05), but a significantly greater reduction was observed to the distal aspect of the roots, compared to the mesial aspect, in both groups (p < .05; Table 3; Figure 4).
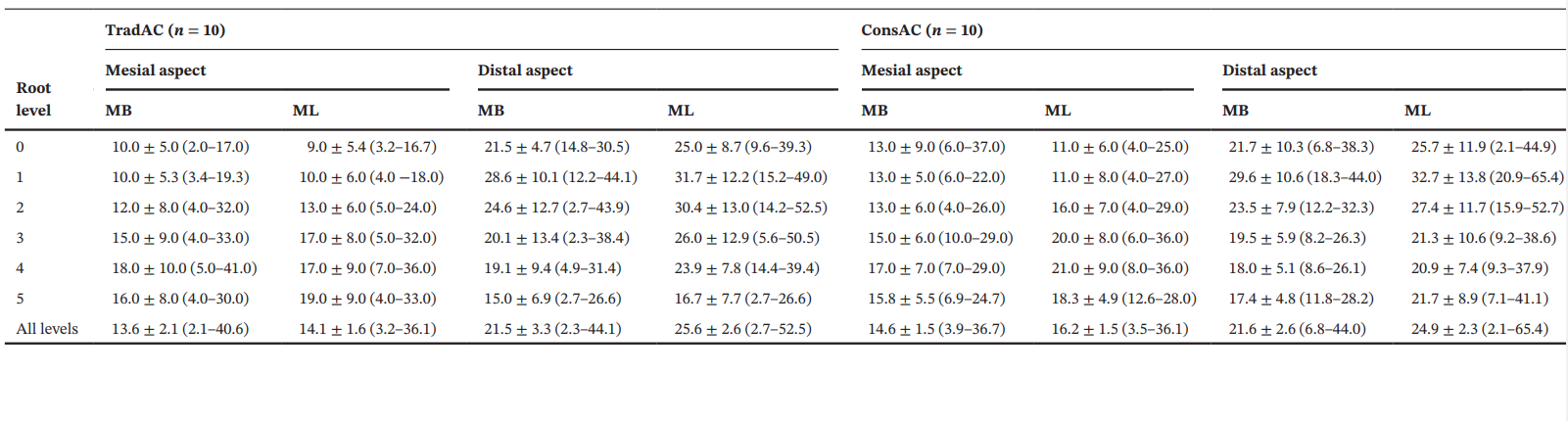
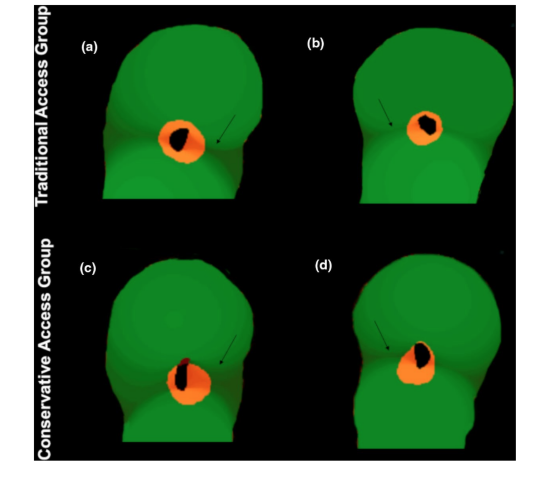
Table 4 depicts the percentage frequency distribution of dentine thickness categories (<0.5 mm; 0.5–1.0 mm; >1.0 mm) obtained by the evaluation of 240 transaxial cross sections of teeth prepared with TradAC or ConsAC.
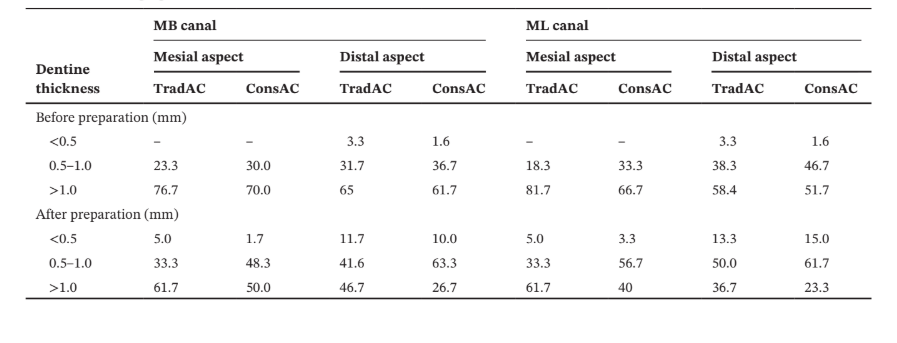
After root canal preparation, dentine thickness thinner than 0.5 mm was observed mostly at the distal aspect of the root (10% to 15%) in the MB and ML canals, with no influence of the access cavity type on its incidence to either mesial (X2 = 1.66; p = .2) or distal (X2 = 0.40; p = .5) directions. In the TradAC group, dentine thickness in most of the slices (n = 124) was greater than 1.0 mm after preparation whilst, in the ConsAC, it ranged from 0.5 to 1.0 mm (n = 136).
Discussion
In the present study, 20 mesial roots of mandibular molars were selected from a pool of teeth, pair matched according to the root canal morphology and distributed into groups according to the type of access cavity preparation: TradAC or ConsAC (Figure 2). The root canals were then enlarged using thermomechanically treated nickel–titanium reciprocating instruments, and hundreds of transaxial cross-sectional slices obtained with high-resolution micro-CT technology were compared for dentine thickness. As would be expected and in line with a previous publication using similar methodology (Keleş et al., 2020), the lowest values of dentine thickness were observed after canal preparation at all evaluated levels of both groups (Table 1; Figure 3). However, no significant difference in the remaining dentine thickness was found between TradAC and ConsAC groups (Table 3), and the null hypothesis was confirmed. These are original results considering that, so far, no research using radiograph, micro-CT or CBCT imaging methods was designed specifically to address this morphological aspect in teeth with different types of access cavity preparation.
In the TradAC and ConsAC groups, the largest percentage reduction in dentine thickness was observed towards the distal direction after preparation of both MB and ML canals (Figure 4). In mandibular molars, the mesial root usually displays an asymmetric shape in its cross section with a deep developmental distal groove (De-Deus et al., 2019; Versiani et al., 2016) that commonly results in dentine thicknesses ranging from 0.5 to 1 mm (Berutti & Fedon, 1992; Keleş et al., 2020), as observed in the present study (Table 4; Figure 3). This thin area at the inner canal walls is considered more prone to strip perforation by the mechanical preparation and was named by Abou-Rass et al. (1980) as the danger zone. However, the concept of thinner dentine walls related only to the distal aspect of the mesial root of mandibular molars has been challenged by Lee et al. (2015) and De-Deus et al. (2019). These authors evaluated hundreds of transaxial root slices acquired by micro-CT technology and reported that in 33% (Lee et al., 2015) and 40% (De-Deus et al., 2019) of the evaluated specimens, the thinnest dentine towards the mesial portion of the root and not the distal (furcation area).
Although it was not the aim of the present study, the position of the thinnest dentine around the MB and ML canal walls also varied in some slices.
In studies using biological samples, some degree of anatomical heterogeneity is always expected. The strength of the present study relies on sample selection and distribution into groups. Preliminary efforts were made to ensure comparability of the groups by anatomically matching the specimens based on morphometric parameters of the root canal system (configuration, length, volume and geometry), which enhanced the internal validity of the method, created a reliable baseline for the experimental procedures and reduced the anatomical bias that would influence the results (De-Deus et al., 2020; Versiani et al., 2013). This approach, combined with the canal enlargement using the same preparation protocol, explains the similarities observed between TradAC and ConsAC groups regarding the percentage frequency reduction in dentine thickness (Table 3). Despite these efforts, in this type of study, it is unfeasible to match real teeth according to their dentine thicknesses at all levels, and these anatomical dissimilarities amongst roots explain their different percentage distributions after canal preparation when slices were categorized according to this aspect (Table 4). Thus, to avoid this limitation, groups were compared regarding the percentage reduction in thickness instead of absolute values. In the future, with the improvement of raw materials, 3D-printed models of teeth based on micro-CT scans would allow the standardization of groups regarding any anatomical aspect that may impact on the outcome of the study.
In contrast with other laboratory models in which teeth are hand-held or fixed in a bench-top apparatus, in this study, extracted teeth were mounted in a dental mannequin and a phantom head to simulate a clinical condition, and operational procedures were performed in an ergonomic working position using an operating microscope. This setup ensures a level of difficulty closer to clinical practice, yielding more reliable results (Augusto et al., 2020; Rover et al., 2020; Silva et al., 2020b). One point of criticism in this study would be the use of a large-tapered instrument as a master apical file for the preparation of mesial canals of mandibular molars considering that this approach is not recommended in minimally invasive endodontics. On the other hand, it is likely that the use of small-tapered and high-flexible instruments would not properly enlarge the canal space to the point that its deflection would be influenced by the access cavity preparation. In spite of the over enlargement of the mesial canals, no instrument fracture, strip perforation or significant deviation of the original canals were observed. These findings can be explained by the regressive taper of the Reciproc Blue R40, which promotes less removal of coronal dentine in comparison to continuously tapered instruments (Almeida et al., 2019), and its high flexibility (De-Deus et al., 2014) provided by the proprietary manufacturing process. Sample selection including relatively straight roots and the volume of interest limited to the most coronal part of the canals also help to explain the results. Besides, a previous enlargement of the root canals with Reciproc R25 reduced the stress over the active part of the R40 instrument preventing excessive transportation. As a result, the access cavity types tested in this study had no influence on the percentage reduction in dentine or on the incidence of dentine thickness less than 0.5 mm to either mesial or distal root directions. Besides, none of the remaining dentine thicknesses measured in both canals at all levels was less than 0.3 mm. This latter aspect is important considering that an extremely thin remaining root canal walls after preparation could be permeable to bacteria and their by-products (Boreak et al., 2015) and compromise the mechanical resistance of teeth (Lim & Stock, 1987).
Although it has been reported that the maximum angle of canal curvature is greater in teeth with ConsAC compared to TradAC (Eaton et al., 2015; Zhang et al., 2019) and the preparation of mesial canals of mandibular molars with ConsAC resulted in a major deviation of the original anatomy because of the excessive pressure of the instrument against the outer aspect of the curvature (Alovisi et al., 2018), in the present study the access cavity type did not influence the remaining dentine thickness at the coronal third of mesial canals. Further studies should evaluate the influence of more ConsAC preparations, such as ultraconservative and truss types, in other groups of teeth using protocols suggested for minimally invasive preparation.
Conclusion
Traditional or conservative access cavity preparations in extracted mandibular molars did not influence the remaining dentine thickness along the coronal third of mesial canals enlarged with thermomechanically treated nickel–titanium reciprocating instruments.
Authors: Emmanuel J. N. L. Silva, Carolina O. Lima, Ana Flávia A. Barbosa, Thiago Moreira, Erick M. Souza, Gustavo De-Deus, Marco A. Versiani
References:
- Abou-Rass, M., Frank, A.L. & Glick, D.H. (1980) The anticurvature filing method to prepare the curved root canal. Journal of the American Dental Association, 101, 792–794.
- Almeida, B.M., Provenzano, J.C., Marceliano-Alves, M.F., Roças, I.N. & Siqueira, J.F. Jr. (2019) Matching the dimensions of currently available instruments with the apical diameters of mandibular molar mesial root canals obtained by microcomputed tomography. Journal of Endodontics, 45, 756–760.
- Alovisi, M., Pasqualini, D., Musso, E., Bobbio, E., Giuliano, C. & Mancino, D. et al. (2018) Influence of contracted endodontic access on root canal geometry: an in vitro study. Journal of Endodontics, 44, 614–620.
- Augusto, C.M., Barbosa, A.F.A., Guimarães, C.C., Lima, C.O., Ferreira, C.M., Sassone, L.M. et al. (2020) A laboratory study of the impact of ultraconservative access cavities and minimal root canal tapers on the ability to shape canals in extracted mandibular molars and their fracture resistance. International Endodontic Journal, 53, 1516–1529.
- Barbosa, A.F.A., Silva, E.J.N.L., Coelho, B.P., Ferreira, C.M.A., Lima, C.O. & Sassone, L.M. (2020) The influence of endodontic access cavity design on the efficacy of canal instrumentation, microbial reduction, root canal filling and fracture resistance in mandibular molars. International Endodontic Journal, 53, 1666–1679.
- Berutti, E. & Fedon, G. (1992) Thickness of cementum/dentin in mesial roots of mandibular first molars. Journal of Endodontics, 18, 545–548.
- Boreak, N., Ishihata, H. & Shimauchi, H. (2015) A photochemical method for in vitro evaluation of fluid flow in human dentine. Archives of Oral Biology, 60, 193–198.
- Clark, D. & Khademi, J.A. (2010a) Modern molar endodontic access and directed dentin conservation. Dental Clinics of North America, 54, 249–273.
- Clark, D. & Khademi, J.A. (2010b) Case studies in modern molar endodontic access and directed dentin conservation. Dental Clinics of North America, 54, 275–289.
- De-Deus, G., Leal Vieira, V.T., Silva, E.J., Lopes, H., Elias, C.N. & Moreira, E.J. (2014) Bending resistance and dynamic and static cyclic fatigue life of Reciproc and WaveOne large instruments.
- Journal of Endodontics, 40, 575–579.
- De-Deus, G., Rodrigues, E.A., Belladonna, F.G., Simões-Carvalho, M., Cavalcante, D.M., Oliveira, D.S. et al. (2019) Anatomical danger zone reconsidered: a micro-CT study on dentine thickness in mandibular molars. International Endodontic Journal, 52, 1501–1507.
- De-Deus, G., Simões-Carvalho, M., Belladonna, F.G., Versiani, M.A., Silva, E.J.N.L., Cavalcante, D.M. et al. (2020) Creation of well-balanced experimental groups for comparative endodontic laboratory studies: a new proposal based on micro-CT and in silico methods. International Endodontic Journal, 53, 974–985.
- Doube, M., Kłosowski, M.M., Arganda-Carreras, I., Cordelières, F.P., Dougherty, R.P., Jackson, J.S. et al. (2010) BoneJ: free and extensible bone image analysis in ImageJ. Bone, 47, 1076–1079.
- Eaton, J.A., Clement, D.J., Lloyd, A. & Marchesan, M.A. (2015) Micro-computed tomographic evaluation of the influence of root canal system landmarks on access outline forms and canal curvatures in mandibular molars. Journal of Endodontics, 41, 1888–1891.
- Garcia Filho, P.F., Letra, A., Menezes, R. & Carmo, A.M. (2003) Danger zone in mandibular molars before instrumentation: an in vitro study. Journal of Applied Oral Science, 11, 324–326.
- Ingle, J.I. (1985) Endodontic cavity preparation. In: Ingle, J. & Tamber, J. (Eds.) Endodontics, 3rd edition. Philadelphia, PA: Lea & Febiger, pp. 102–167.
- Keleş, A., Keskin, C., Alqawasmi, R. & Versiani, M.A. (2020) Evaluation of dentine thickness of middle mesial canals of mandibular molars prepared with rotary instruments: a micro-CT study. International Endodontic Journal, 53, 519–528.
- Kessler, J.R., Peters, D.D. & Lorton, L. (1983) Comparison of the relative risk of molar root perforations using various endodontic instrumentation techniques. Journal of Endodontics, 9, 439–447.
- Lee, J.K., Yoo, Y.J., Perinpanayagam, H., Ha, B.H., Lim, S.M., Oh, S.R. et al. (2015) Three-dimensional modelling and concurrent measurements of root anatomy in mandibular first molar mesial roots using micro-computed tomography. International Endodontic Journal, 48, 380–389.
- Lim, S.S. & Stock, C.J. (1987) The risk of perforation in the curved canal: anticurvature filing compared with the stepback technique. International Endodontic Journal, 20, 33–39.
- Lima, C.O., Barbosa, A.F.A., Ferreira, C.M., Ferretti, M.A., Aguiar, F.H.B., Lopes, R.T. et al. (2021) Influence of ultraconservative access cavities on instrumentation efficacy with XP-endo Shaper and Reciproc, filling ability and load capacity of mandibular molars subjected to thermomechanical cycling. International Endodontic Journal, 54, 1383–1393.
- Montgomery, S. (1985) Root canal wall thickness of mandibular molars after biomechanical preparation. Journal of Endodontics, 11, 257–263.
- Nagendrababu, V., Murray, P.E., Ordinola-Zapata, R., Peters, O.A., Rôças, I.N., Siqueira, J.F. et al. (2021) PRILE 2021 guidelines for reporting laboratory studies in Endodontology: a consensus-based development. International Endodontic Journal, 54, 1482–1490.
- Neelakantan, P., Khan, K., Hei, G.P., Yip, C.Y., Zhang, C. & Pan Cheung, G.S. (2018) Does the orifice-directed dentin conservation access design debride pulp chamber and mesial root canal systems of mandibular molars similar to a traditional access design? Journal of Endodontics, 44, 274–279.
- Patel, S. & Rhodes, J. (2007) A practical guide to endodontic access cavity preparation in molar teeth. British Dental Journal, 203, 133–140.
- Pedullà, E., La Rosa, G.R.M., Boninelli, S., Rinaldi, O.G., Rapisarda, E. & Kim, H.C. (2018) Influence of different angles of file access on cyclic fatigue resistance of Reciproc and Reciproc Blue instruments. Journal of Endodontics, 44, 1849–1855.
- Rover, G., Belladonna, F.G., Bortoluzzi, E.A., De-Deus, G., Silva, E.J.N.L. & Teixeira, C.S. (2017) Influence of access cavity design on root canal detection, instrumentation efficacy, and fracture resistance assessed in maxillary molars. Journal of Endodontics, 43, 1657–1662.
- Rover, G., Lima, C.O., Belladonna, F.G., Garcia, L.F.R., Bortoluzzi, E.A., Silva, E.J.N.L. et al. (2020) Influence of minimally invasive endodontic access cavities on root canal shaping and filling ability, pulp chamber cleaning and fracture resistance of extracted human mandibular incisors. International Endodontic Journal, 53, 1530–1539.
- Silva, A.A., Belladonna, F.G., Rover, G., Lopes, R.T., Moreira, E.J.L., De-Deus, G. et al. (2020b) Does ultraconservative access affect the efficacy of root canal treatment and the fracture resistance of two-rooted maxillary premolars? International Endodontic Journal, 53, 265–275.
- Silva, E., Pinto, K.P., Ferreira, C.M., Belladonna, F.G., De-Deus, G., Dummer, P. et al. (2020a) Current status on minimal access cavity preparations: a critical analysis and a proposal for a universal nomenclature. International Endodontic Journal, 53, 1618–1635.
- Versiani, M.A., Ordinola-Zapata, R., Keleş, A., Alcin, H., Bramante, C.M., Pécora, J.D. et al. (2016) Middle mesial canals in mandibular first molars: a micro-CT study in different populations. Archives of Oral Biology, 61, 130–137.
- Versiani, M.A., Pécora, J.D. & Sousa-Neto, M.D. (2013) Microcomputed tomography analysis of the root canal morphology of single-rooted mandibular canines. International Endodontic Journal, 46, 800–807.
- Vieira, G.C.S., Pérez, A.R., Alves, F.R.F., Provenzano, J.C., Mdala, I., Siqueira, J.F. et al. (2020) Impact of contracted endodontic cavities on root canal disinfection and shaping. Journal of Endodontics, 46, 655–661.
- Zhang, Y., Liu, Y., She, Y., Liang, Y., Xu, F. & Fang, C. (2019) The effect of endodontic access cavities on fracture resistance of first maxillary molar using the extended finite element method. Journal of Endodontics, 45, 316–321.