
Worldwide Assessment of the Mandibular First Molar Second Distal Root and Root Canal: A Cross-sectional Study with Meta-analysis
Abstract
Introduction: This study assessed the prevalence of radix entomolaris and 2 canals at the distal aspect of mandibular first molars among different geographic regions by means of cone- beam computed tomographic imaging.
Methods: Precalibrated observers from 23 worldwide geographic locations followed a standardized screening protocol to assess 5750 cone-beam computed tomographic images of mandibular first molars (250 per region), gathering demographic data and recording the presence of radix entomolaris and a second canal at the distal aspect of teeth. Intra- and interrater reliability tests were conducted and comparisons among groups were performed using proportions and odds ratio forest plots. The significance level was set at 5%.
Results: The results of intra- and interrater tests were above 0.79. The prevalence of radix entomolaris varied from 0.9% in Venezuela (95% confidence interval [CI], 0%–1.9%) to 22.4% in China (95% CI, 17.2%–27.6%). Regarding the proportion of a second distal canal, it ranged from 16.4% in Venezuela (95% CI, 11.8%– 21.0%) to 60.0% in Egypt (95% CI, 53.9%–66.1%). The East Asia subgroup was associated with a significantly higher prevalence of an extra distolingual root, whereas the American subgroup, the American native ethnic group, and elderly patients were linked to significantly lower percentages of a second canal at the distal aspect of teeth. No significant differences were noted between male or female patients.
Conclusions: The overall worldwide prevalence rates of radix entomolaris and a second canal at the distal aspect of the mandibular first molar were 5.6% and 36.9%, respectively. The East Asia geographic region and Asian ethnic group had a higher prevalence of a second distal root. (J Endod 2021;■:1–11.)
The clinical relevance of knowing the root canal system morphology and being able to identify the most common configurations and variations has been recognized for years, being 1 of the most important research topics in endodontics. With the widespread implementation of cone-beam computed tomographic (CBCT) imaging as an adjunctive diagnostic aid in clinical practice, the evaluation of root canal configurations has become more precise. This imaging technology has been used in cross-sectional in vivo studies to evaluate the prevalence of missed canals in endodontically treated teeth. After screening thousands of CBCT scans, authors identified a high prevalence of missed canals in molars, most of them associated with apical periodontitis. For example, Karabucak et al and Costa et al noted missed canals in 19.7% and 18.5% of mandibular first molars, respectively, whereas Baruwa et al not only observed missed canals in 11.1% of these teeth (95% of them with periapical lesion) but also assessed each root and reported a higher frequency of missed canals in the distal root compared with the mesial ones.
The root canal system of the mandibular first molar is 1 of the most challenging to properly clean and shape because of its morphologic unpredictability.
Notwithstanding, a variety of canal configurations have been described in this group of teeth; the mesial root has been capturing more interest over the years because of its more complex and unpredictable anatomy, which includes the presence of a danger zone9, isthmuses, extra canals, or complex apical morphologies, whereas the distal root has been relegated to a secondary level of interest despite the available specific literature.
Another important variation that can be found in this group of teeth is the presence of an extra root at its distolingual aspect, the so-called radix entomolaris. Although this extra root has been correlated to a significant ethnic trait in Asian countries such as China and Korea, uncertainty still exists regarding its prevalence in other regions of the globe. Moreover, it is currently unknown if the prevalence of a second root canal at the distal aspect of mandibular first molars is also more common in regions with higher proportions of radix entomolaris, corroborating this ethnic trait. Therefore, the objectives of this cross-sectional in vivo study were the assessment of the worldwide prevalence of a second distal root and a second distal canal in mandibular first molars using CBCT images and the evaluation of the impact of some demographic data on the outcomes. The null hypotheses to be tested were that there were no differences regarding the proportions of an (1) extra distal root and (2) two distal root canals among different geographic regions around the globe.
Materials and methods
Study Outcomes, Sample Size Calculation, and Research Protocol
The prevalence of the radix entomolaris (primary outcome) and the proportion of a second canal at the distal aspect of the tooth (secondary outcome) in permanent mandibular first molars were determined by 23 specialists in endodontics from 23 geographic regions of 5 continents. Data were acquired by assessing preexisting CBCT volumes in accordance with the position statement of the American Association of Endodontists. All observers were calibrated simultaneously with written instructions regarding the CBCT screening methodology, anatomic landmark definitions, exemplification through CBCT images, research deadlines, bibliographic references, and a tutorial video showing the step-by-step protocol to be followed. Sample size was calculated taking into consideration a previous cross-sectional in vivo CBCT study in which 2 geographic regions (included in the current research) were compared regarding the prevalence of a distolingual root in mandibular first molars. A total of 32 patients were determined considering a confidence level of 95%, a power of 80%, and an effect size of 23.3. To counterbalance that a calculation was not performed for all regions, the sample size was increased to 250 patients per region. This study protocol followed the guidelines recommended for epidemiologic cross-sectional studies on root and root canal anatomy using CBCT technology and was previously reviewed and approved by the local ethics committee (Comissão de E´tica para a Saúde, Faculdade de Medicina Dentária, Universidade de Lisboa).
Sample Selection, Data Acquisition, and Screening Method
A convenience sample made up of patients attending health centers from the assessed regions was included in the present study. Each observer was instructed to review preexisting CBCT data sets on a consecutive manner following the chart order (alphabetic or numeric) until the determined sample size (N = 250) was achieved while also collecting demographic data such as age and sex.
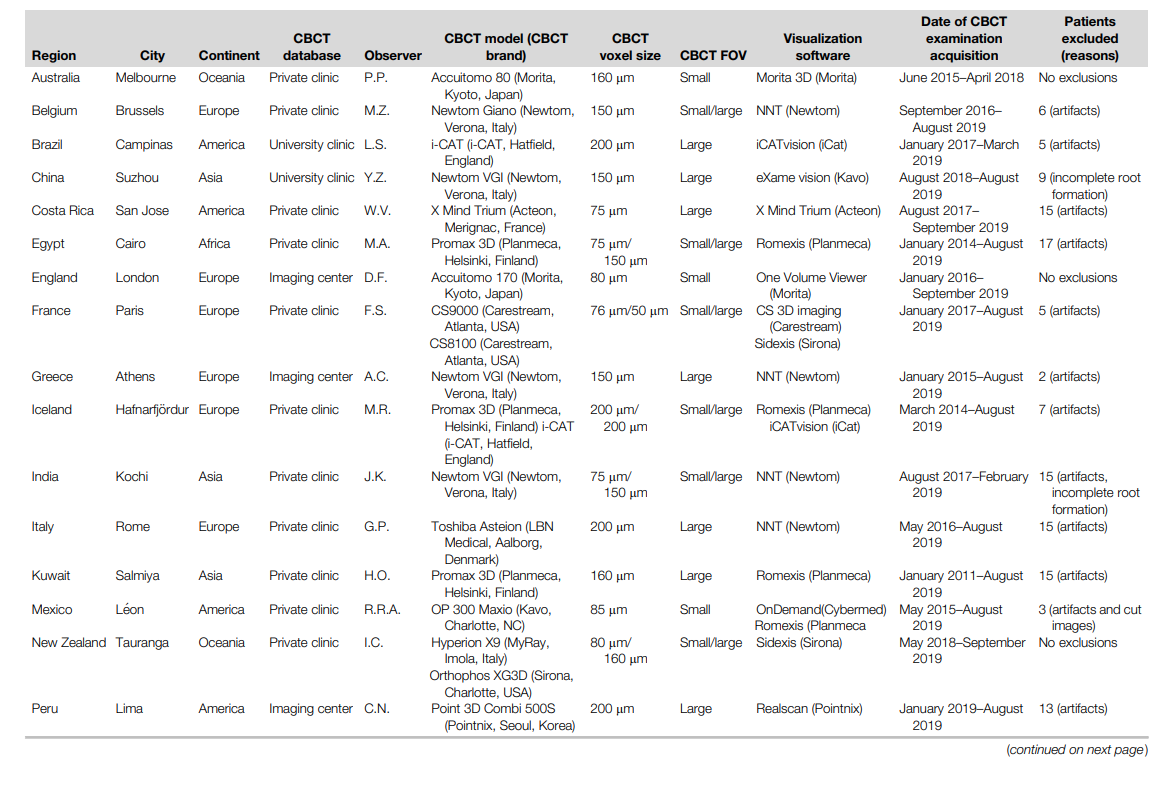
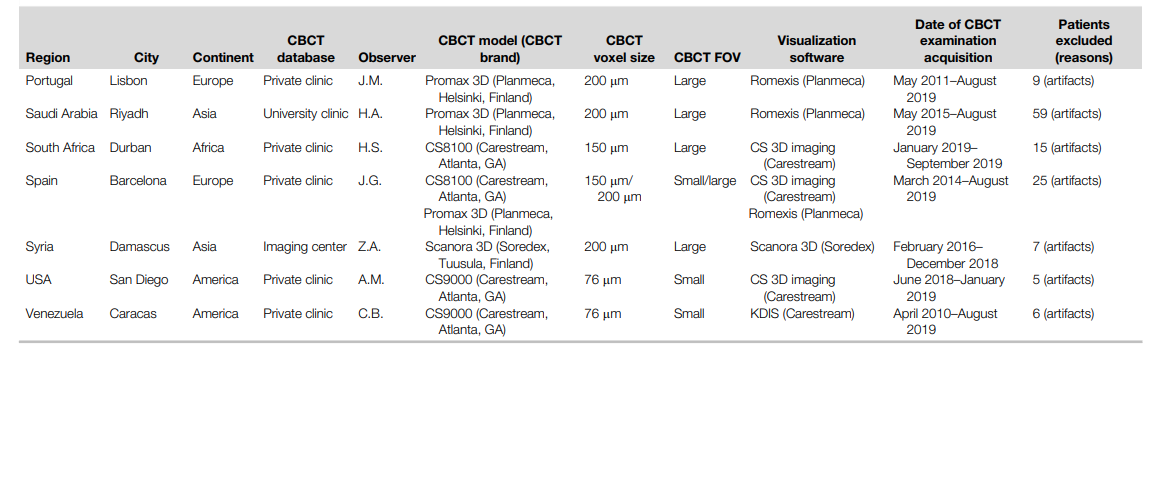
Although only 1 observer was allowed per region, more than 1 CBCT scanner was accepted as long as the voxel size was equal to or under 200 mm. The exclusion criteria included teeth with previous root canal treatment, uncertainty regarding the tooth numbering, incomplete root formation or root resorption, unsalvageable roots, lack of demographic information, and compromised visualization due to imaging artifacts. A total of 253 patients were excluded, representing 6.1% of the assessed population (Table 1).
The CBCT imaging screening method consisted of the assessment of the mandibular first molar distal root(s) in 3 planes (coronal, sagittal, and axial) after the 3-dimensional alignment of the long axis of the root(s) with the reference lines of the visualization software. All observers were allowed to manipulate the visualization settings and tools (such as noise reduction or specific filters) in order to improve the output image quality. The following information was recorded for each mandibular molar:
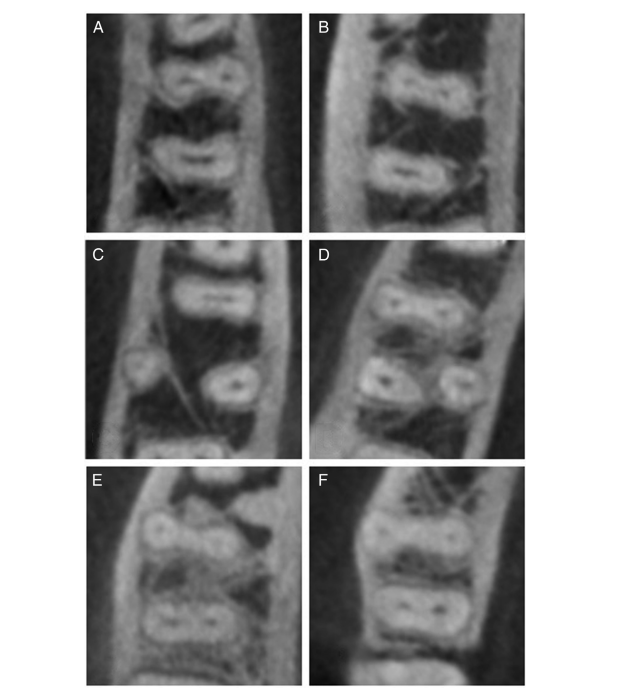
- Primary outcome: the presence of the radix entomolaris (yes/no) identified according to the description reported by Calberson et al. An apical split of the distal root was considered an anatomic feature and not a multirooted configuration (Fig. 1A–F).
- Secondary outcome: the presence of 2 canals at the distal aspect of the tooth (yes/no). In case multiple distal roots were present (traditional distal root 1 radix), the sum of all root canals from all roots were taken into consideration and classified into single canal, 2 independent canals, 2 confluent canals (2 separate canals leaving the pulp chamber but merging into a single one at the apex), or more than 2 root canals (Fig. 1).
If doubts existed regarding the canal configuration, the observers were instructed to consult the research coordinator (J.M.) so a consensus could be reached. All observers were blinded regarding the results from other regions to avoid influence bias on their interpretations. All received information was included into a single sheet in order to allow a nonconformities check (conducted by the study coordinator) and further export to a statistical software program.
Observers’ Intra- and Interreliability
Intra- and interobserver reliability tests were conducted before data acquisition. The former was performed by comparing the scores of 2 evaluations conducted on the same data set within a 1-month interval. In each region, a total of 30 mandibular first molars (12% of all sample) were screened twice regarding the primary outcome. The Cohen kappa value was used to measure each rater reliability. For interobserver reliability, 18 molars from 10 CBCT data sets (not included in any regional data set) were evaluated regarding the primary outcome. The intraclass correlation coefficient (ICC) and percentage of agreement were used to measure the group reliability. Additionally, each individual result was compared with a consensus classification obtained by 2 experienced external evaluators using the Cohen kappa test. A result of 0.60 for both ICC and the Cohen kappa value was defined as the lower limit. The raters were asked to review the study protocol and to repeat the evaluations in case this limit was not reached. Both intra- and interobserver analyses followed the preestablished CBCT screening protocol and were conducted during the same time interval by all raters.
Statistical Analysis
Considering the multicenter nature of this research, a meta-analysis based on a random effects model was performed using the OpenMeta[Analyst] v.10.10 software (http:// www.cebm.brown.edu/openmeta/). The results of both primary (the prevalence of a second distal root) and secondary (the proportion of a second distal canal) outcomes were expressed as odds ratios and untransformed proportions with 95% confidence interval (CI) forest plots. Possible sources of heterogeneity were analyzed through meta-regression. The statistical significance level was set at P ˂ .05.
Results
The kappa values of intra- and interobserver agreement tests regarding the primary outcome were above 0.79 for all observers (Supplemental Table S1 is available online at www.jendodon.com), whereas the ICC and overall agreement scores were 0.999 and 99.8%, respectively.
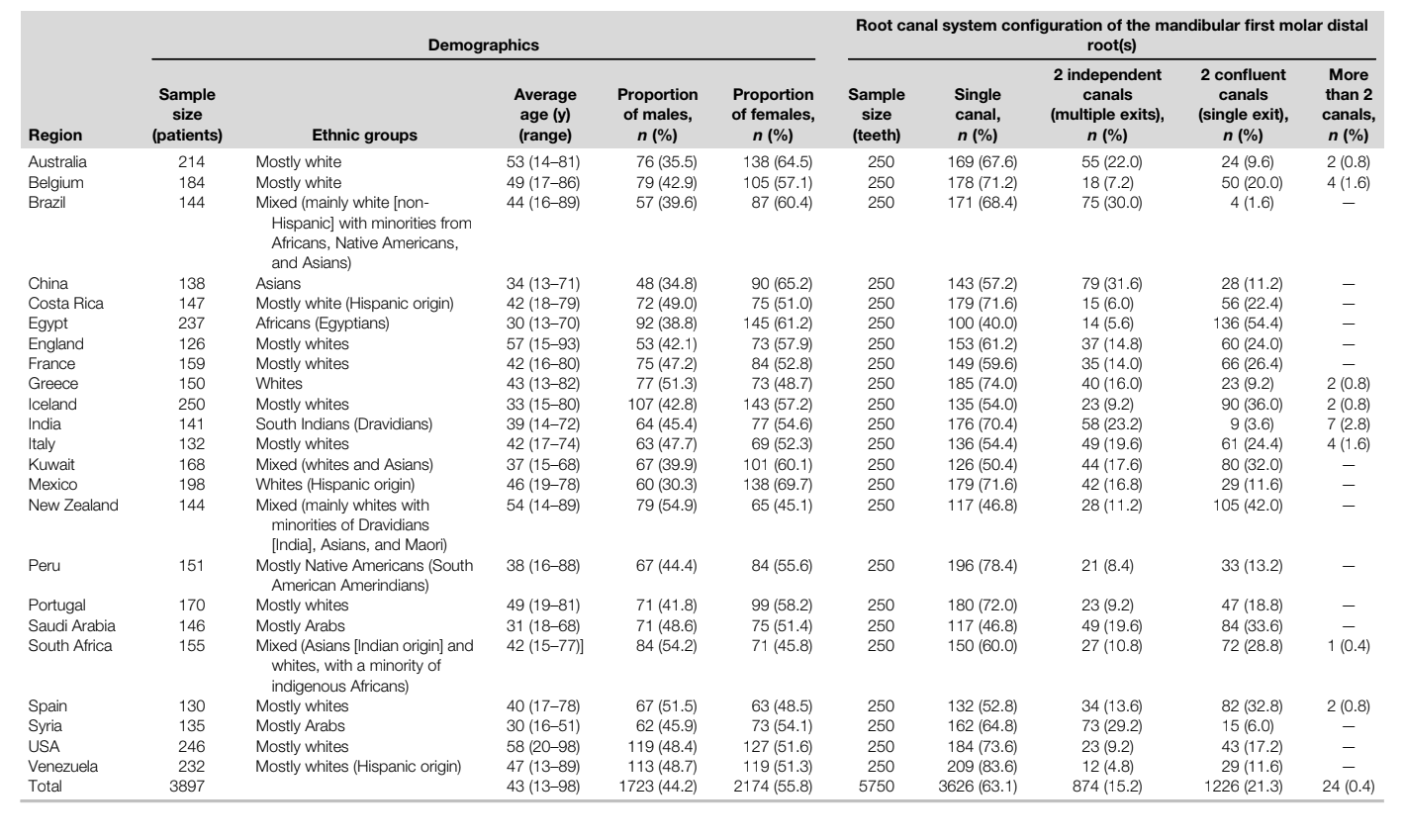
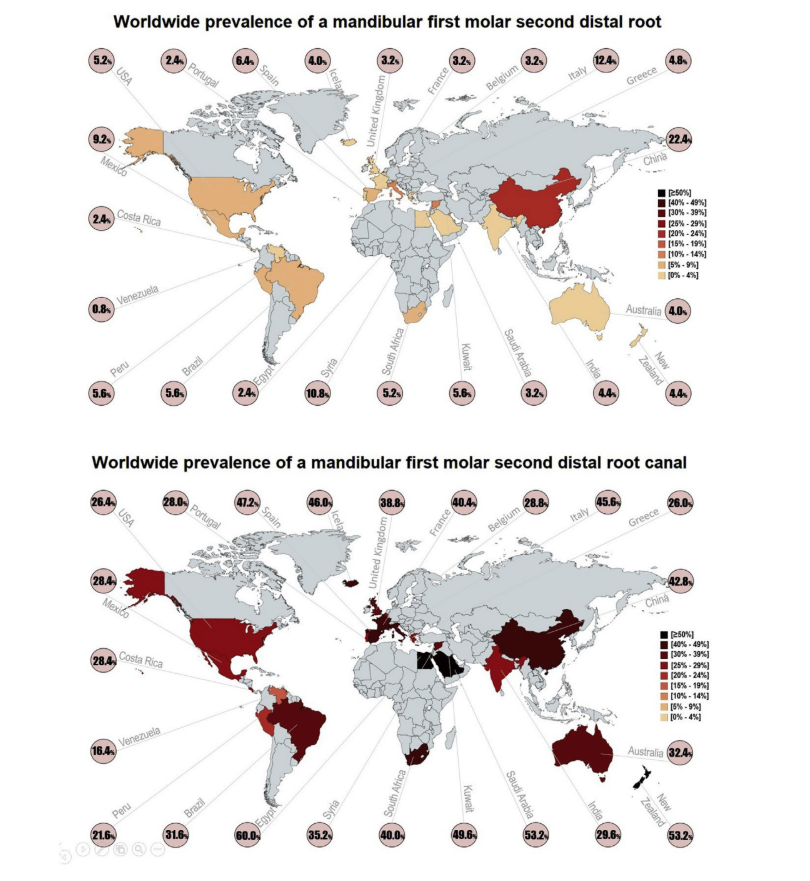
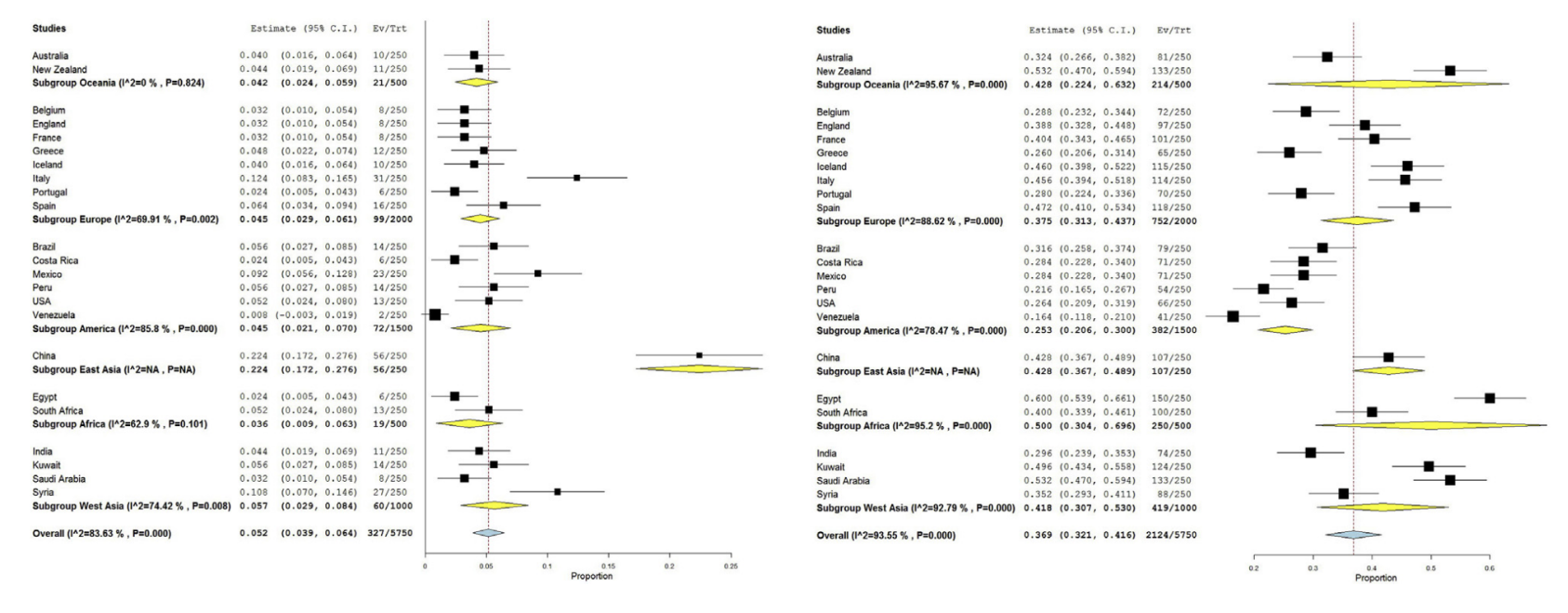
The final sample included 5750 permanent molars from 3897 patients (1723 males and 2174 females) with a mean age of 43 years (Table 2). The overall worldwide prevalence of radix entomolaris was 5.6% (95% CI, 4.3%–6.9%), ranging from 0.9% in Venezuela (95% CI, 0%–1.9%) to 22.4% in China (95% CI, 17.2%–27.6%), whereas the prevalence of 2 canals at the distal aspect of the tooth was 36.9% (95% CI, 32.1%–41.6%), varying from 16.4% in Venezuela (95% CI, 11.8%–21.0%) to 60.0% in Egypt (95% CI, 53.9%–66.1%) (Fig. 2). When a multiple canal system was observed in the tooth distal aspect, the most common configuration was 2 confluent canals (21.3%) (Table 2).
Considering the results obtained from different voxel sizes (from 75–200 mm), an almost constant prevalence of both second distal roots and canals were observed in the CBCT imaging voxel meta-regression (Supplemental Fig. S1 is available online at www.jendodon.com), and the heterogeneity of the results could not be explained by the voxel size (omnibus P values = .070 [second root] and .060 [second canal]).
A significantly higher prevalence of radix entomolaris was observed in the East Asian region (22.4% [95% CI, 17.2%–27.6%]) compared with other regions (P ˂ .05) that showed no difference among them (P ˃ .05) and whose percentages ranged from 3.6% in Africa (0.9%-6.3%, CI 95%) to 5.7% in West Asia (95% CI, 2.9%–8.4%). The prevalence of a second canal at the distal aspect of the teeth ranged from 25.3% in America (95% CI, 20.6%–30.0%) to 50.0% in Africa (95% CI, 30.4%–69.6%), a difference considered statistically significant (P ˂ .05). Other significant differences were also noted among regions and are depicted in Figure 3.
The analysis of ethnic groups confirmed that Asians had a significantly higher proportion of radix entomolaris than other regions (P ˂ .05), whereas a mixed pattern for the proportions of a second distal canal was noted, with the lowest and highest values observed in native Americans (21.6% [95% CI, 16.5%–26.7%]) and Africans (60.0% [95% CI, 53.9%–66.1%]), respectively (P ˂ .05) (Supplemental Fig. S2 is available online at www.jendodon.com). The results according to sex were balanced without any statistical difference regarding the proportions (Supplemental Fig. S3 is available online at www.jendodon.com) or odds ratio (Supplemental Fig. S4 is available online at www.jendodon.com) (P ˃ .05). The analysis of groups according to age revealed that the prevalence of 2 canals at the distal aspect of the tooth in elderly patients (˃61 years: 31.0% [95% CI, 27.9%–34.1%]) was significantly lower (P ˂ .05) (Supplemental Fig. S5 is available online at www.jendodon.com).
Discussion
Although several approaches have been used to study the morphology of teeth, in the last decade nondestructive methods such as micro–computed tomographic and CBCT imaging have been the most used. Although studies using micro–computed tomographic imaging take advantage of its superior resolution to focus on pure anatomic descriptions and morphometric measurements, CBCT studies explore the possibility of assessing in vivo characteristics of large populations in order to evaluate the influence of some demographic factors in the prevalence of a particular morphologic feature. Both imaging modalities are essential to understand the anatomy of teeth because each has specificities that allow answering specific questions depending on the study’s proposal. The present research intended to determine the worldwide prevalence of radix entomolaris and a second canal in the distal aspect of mandibular first molars by screening 5750 CBCT images through a dichotomous response (presence/absence) and to evaluate the influence of some demographic factors on these outcomes. Overall, the analysis of the results showed significant differences among different geographic regions, and the null hypotheses were rejected.
In the literature, the reported prevalence of radix entomolaris was higher in some Asian subpopulations, including Taiwanese (25.3%), Koreans (25.8%), and Chinese (29.3%). These percentages are much higher than the ones reported in Europe (2.6% in Portugal, 2.8% in Belgium, and 4.1% in Spain), South America (1.5% in Brazil and 6.2% in Chile), and the Middle East (0.5% in Turkey and 3.1% in Iran). The present study assessed several regions that had never been studied before and, in agreement with previous publications, found a significantly higher prevalence of radix entomolaris only in China (22.4%), whereas the combined proportion of the other 22 regions was only 4.9% (Fig. 3). However, this higher risk factor of radix entomolaris in China was not followed by a higher prevalence of an extra distal canal (42.8%) (Figs. 2 and 3). Actually, the present findings show that the highest prevalence of a second distal canal was not in Asian populations (42.8%) but rather in African populations (40.0%–60.0%). Interestingly, this outcome corroborates with the high prevalence of extra canals reported in other groups of teeth in Africans such as the second mesiobuccal canal in maxillary first molars and the lingual canal in mandibular first premolars. Additionally, the global proportion of a second distal canal in mandibular first molars in America was 25.3% (lowest) (Fig. 3); the present results confirmed previous lower frequencies reported in some American subpopulations as in Brazil (23.4%), whereas other regions present higher proportions, such as Europe (27.7% and 29.2%) and China (20.5%, 22.7%, and 37.1%).
Regarding the influence of demographic factors on the outcomes, it was possible to observe that the analysis of ethnic groups somehow paired the results of geographic regions because of the strong presence of certain ethnic groups in specific regions, such as the case of Asian patients represented only by the East Asia subgroup (Fig. 3, Supplemental Fig. S2 is available online at www.jendodon.com). On the other hand, sex had no influence on the outcomes when assessed through proportions or odds ratio forest plots (Supplemental Figs. S3 and S4 are available online at www.jendodon.com). The analysis of age groups was conducted only for the second distal canal because roots are not expected to change over time. Younger groups were associated with higher proportions of 2 distal root canals compared with the elderly ones (Supplemental Fig. S5 is available online at www.jendodon.com), a finding that may be partially explained by the dentin deposition over the years due to physiological and pathologic stimuli. Notwithstanding that the analysis of the age factor contradicts previous findings on this root, it corroborates with the data observed in other groups of teeth.
From an anthropological point of view, radix entomolaris in mandibular first molars is considered an ethnic trait. Previous anthropological studies have investigated several crown traits related to this particular tooth, such as the pit-tubercle or additional cusps. The limited information related to root traits suggests that potential differences among Neanderthals and anatomically modern humans might be related to distinct occlusal function regimens. However, a hypothesis that may help to partly explain this anatomic variation mostly in Asian populations was provided by investigations conducted on lower jaws from Denisovan hominins found in a cave in Xiahe County, Tibet, in 1980. This study associated the 3-rooted configuration of mandibular molars to extinct subspecies of archaic humans who have lived mostly in Siberia while spreading for other East Asia regions and shared the geographic area (where they lived) during the Paleolithic period with 2 other hominids: the Homo sapiens and Neanderthals. Genome comparison also suggests an interbreeding of D. hominins with early modern humans and Neanderthals.
This heritage, passed via gene flow from the Denisovans to their East Asian hybrid descendants, might explain why the second root trait remained more restricted to regions such as China and Korea and did not spread all around the world during human world colonization, including the passage of early humans from Asia to North America or Oceania.
The main limitations of the present study include potential bias related to the observer, the local CBCT scanner, and the visualization software. Regarding the observer, several efforts were conducted to provide them with relevant information through the same pathway and timetable while setting the outcomes at a dichotomous level (presence/absence). This approach ultimately led to highly favorable results in 3 different rater reliability tests. Regarding the CBCT scanner, a maximum voxel size limit was set at 200 mm. This size has been shown to be a limit that does not influence the results compared with lower sizes, and a meta-regression analysis was unable to identify any source of bias related to this factor (Supplemental Fig. S1 is available online at www.jendodon.com). The multiple visualization software used in different regions not only had similar features but also allowed similar outcomes, mostly because this study focused in evaluating only major structures and provided only a dichotomous response. This approach favored the assessment through any specialized software in different regions. The main strength of the present research was its multicentered nature, including multiple regions around the globe, and the assessment of a large number of teeth (N = 5750). Additionally, the meta-analysis statistical comparisons were possible in order to explore differences, confounders, and heterogeneities, as previously performed, because of the methodological standardization of the screening protocol for all regions. Taken together, multiple factors such as the in vivo approach, the large sample size, the multicentered assessment, and the robust statistical analysis increase the reliability of the present results. Further studies should explore other geographic regions and morphologic variations of roots and root canals based on sound and innovative methodologies to provide new demographic and anthropological data.
Conclusions
The overall worldwide prevalence rates of radix entomolaris and a second canal at the distal aspect of mandibular first molars were 5.6% and 36.9%, respectively. Demographic characteristics such as geographic region, ethnicity, and age groups influenced the outcomes, whereas sex had no impact.
Authors: Jorge N. R. Martins, Christian Nole, Hani F. Ounsi, Peter Parashos, Gianluca Plotino, Magnus F. Ragnarsson, Ruben Rosas Aguilar, Fabio Santiago, Hussein C. Seedat, Walter Vargas, Murilo von Zuben, Yuerong Zhang, Hussam Alfawaz, Moataz-Bellah A. M. Alkhawas, Zaher Altaki, Luiza Berti, Carlos Boveda, Imran Cassim, Antonis Chaniotis, Daniel Flynn, Jose Antonio Gonzalez, Jojo Kottoor, Adam Monroe, Emmanuel J. N. L. Silva and Marco Aurelio Versiani
References:
- Baruwa AO, Martins JN, Meirinhos J, et al. The influence of missed canals on the prevalence of periapical lesions in endodontically treated teeth: a cross-sectional study. J Endod 2020;46:34–9.
- Costa F, Pacheco-Yanes J, Siqueira JF, et al. Association between missed canals and apical periodontitis. Int Endod J 2019;52:400–6.
- Karabucak B, Bunes A, Chehoud C, et al. Prevalence of apical periodontitis in endodontically treated premolars and molars with untreated canal: a cone-beam computed tomography study. J Endod 2016;42:538–41.
- Gu Y, Lu Q, Wang H, et al. Root canal morphology of permanent three-rooted mandibular first molars-part I: pulp floor and root canal system. J Endod 2010;36:990–4.
- Kim SY, Kim BS, Woo J, Kim Y. Morphology of mandibular first molars analyzed by cone-beam computed tomography in a Korean population: variations in the number of roots and canals. J Endod 2013;39:1516–21.
- Martins JN, Marques D, Silva E, et al. Prevalence studies on root canal anatomy using cone- beam computed tomographic imaging: a systematic review. J Endod 2019;45:372–86.
- de Pablo OV, Estevez R, Peix Sanchez M, et al. Root anatomy and canal configuration of the permanent mandibular first molar: a systematic review. J Endod 2010;36:1919–31.
- Versiani M, Pereira MR, Pecora JD, Sousa-Neto MD. Root canal anatomy of maxillary and mandibular teeth. In: Versiani M, Basrani B, Sousa-Neto MD, editors. The Root Canal Anatomy in Permanent Dentition; 2019. p. 181–240. Springer International Publishing.
- De-Deus G, Rodrigues EA, Belladonna FG, et al. Anatomical danger zone reconsidered: a micro- CT study on dentine thickness in mandibular molars. Int Endod J 2019;52:1501–7.
- Fan B, Pan Y, Gao Y, et al. Three-dimensional morphologic analysis of isthmuses in the mesial roots of mandibular molars. J Endod 2010;36:1866–9.
- Versiani MA, Ordinola-Zapata R, Keles A, et al. Middle mesial canals in mandibular first molars: a micro-CT study in different populations. Arch Oral Biol 2016;61:130–7.
- Filpo-Perez C, Bramante CM, Villas-Boas MH, et al. Micro-computed tomographic analysis of the root canal morphology of the distal root of mandibular first molar. J Endod 2015;41:231–6.
- Calberson FL, De Moor RJ, Deroose CA. The radix entomolaris and paramolaris: clinical approach in endodontics. J Endod 2007;33:58–63.
- Perez-Heredia M, Ferrer-Luque CM, Bravo M, et al. Cone-beam computed tomographic study of root anatomy and canal configuration of molars in a spanish population. J Endod 2017;43:1511–6.
- Martins JN, Gu Y, Marques D, et al. Differences on the root and root canal morphologies between Asian and White ethnic groups analyzed by cone-beam computed tomography. J Endod 2018;44:1096–104.
- Park JB, Kim N, Park S, et al. Evaluation of root anatomy of permanent mandibular premolars and molars in a Korean population with cone-beam computed tomography. Eur J Dent 2013;7:94–101.
- AAE and AAOMR joint position statement: use of cone beam computed tomography in endodontics 2015 update. Oral Surg Oral Med Oral Pathol Oral Radiol 2015;120:508–12.
- Martins JN, Kishen A, Marques D, et al. Preferred reporting items for epidemiologic cross- sectional studies on root and root canal anatomy using cone-beam computed tomographic technology: a systematized assessment. J Endod 2020;46:915–35.
- Basagana X, Pedersen M, Barrera-Gomez J, et al. Analysis of multicentre epidemiological studies: contrasting fixed or random effects modelling and meta-analysis. Int J Epidemiol 2018;47:1343–54.
- Huang CC, Chang YC, Chuang MC, et al. Evaluation of root and canal systems of mandibular first molars in Taiwanese individuals using cone-beam computed tomography. J Formos Med Assoc 2010;109:303–8.
- Zhang R, Wang H, Tian YY, et al. Use of cone-beam computed tomography to evaluate root and canal morphology of mandibular molars in Chinese individuals. Int Endod J 2011;44:990–9.
- Torres A, Jacobs R, Lambrechts P, et al. Characterization of mandibular molar root and canal morphology using cone beam computed tomography and its variability in Belgian and Chilean population samples. Imaging Sci Dent 2015;45:95–101.
- Caputo BV. Estudo da tomografia computadorizada de feixe co^nico na avaliaç~ao morfolo´gica de raizes e canais dos molares e pre´ molares da populaça~o brasileira [PhD thesis]. Sa~o Paulo, Brazil: Universidade de Sa~o Paulo; 2014.
- Nur BG, Ok E, Altunsoy M, et al. Evaluation of the root and canal morphology of mandibular permanent molars in a south-eastern Turkish population using cone-beam computed tomography. Eur J Dent 2014;8:154–9.
- Rahimi S, Mokhtari H, Ranjkesh B, et al. Prevalence of extra roots in permanent mandibular first molars in Iranian population: a CBCT analysis. Iran Endod J 2017;12:70–3.
- Martins JN, Marques D, Silva EJ, et al. Second mesiobuccal root canal in maxillary molars - a systematic review and meta-analysis of prevalence studies using cone beam computed tomography. Arch Oral Biol 2020;113:104589.
- Martins JN, Zhang Y, von Zuben M, et al. Worldwide prevalence of a lingual canal in mandibular premolars: a multicenter cross-sectional study with meta-analysis. J Endod 2021;47:1253–64.
- Wang Y, Zheng QH, Zhou XD, et al. Evaluation of the root and canal morphology of mandibular first permanent molars in a western Chinese population by cone-beam computed tomography. J Endod 2010;36:1786–9.
- Thomas RP, Moule AJ, Bryant R. Root canal morphology of maxillary permanent first molar teeth at various ages. Int Endod J 1993;26:257–67.
- Martins JN, Ordinola-Zapata R, Marques D, et al. Differences in root canal system configuration in human permanent teeth within different age groups. Int Endod J 2018;51:931–41.
- Weets J. A promising mandibular molar trait in ancient populations of Ireland. Dent Anthropol 2009;22:65–72.
- Townsend G, Yamada H, Smith P. Expression of the entoconulid (sixth cusp) on mandibular molar teeth of an Australian aboriginal population. Am J Phys Anthropol 1990;82:267–74.
- Kupczik K, Hublin JJ. Mandibular molar root morphology in Neanderthals and late Pleistocene and recent Homo sapiens. J Hum Evol 2010;59:525–41.
- Chen F, Welker F, Shen CC, et al. A late Middle Pleistocene Denisovan mandible from the Tibetan Plateau. Nature 2019;569:409–12.
- Pennisi E. Human evolution. More genomes from Denisova Cave show mixing of early human groups. Science 2013;340:799.