
Micro-CT Study of the In Vivo Accuracy of a Wireless Electronic Apex Locator
Abstract
Introduction: This study aimed to compare the in vivo accuracy of Wirele-X and RootZX II electronic apex locators (EALs) in determining the position of the major foramen using micro–computed tomography (micro-CT) as the analytical tool.
Methods: Eleven vital teeth planned for extraction from 5 patients were used. After conventional access cavity preparation, root canals were flared and negotiated up to the apical third with sizes 08 and 10 K-files followed by irrigation with 2.5% NaOCl. K-type files were used to determine the working length of the selected canals using Root ZX II and Wirele-X apex locators until their numeric displays read “0.0.” After fixing the silicon stop to the file, teeth were extracted and imaged in a micro-CT device using a double-scan protocol. Image stacks, with and without the file in the root canal, were then co-registered and the measurement error calculated as the absolute difference between the tip of the file and the major foramen. Positive and negative values were recorded when the file tip was detected beyond or short of the major foramen, respectively. Accuracy was determined on stable measurements within ± 0.5 mm when the file tip did not extend beyond the major foramen. The χ² test was applied to compare the ability of the EALs to detect the position of the major foramen, and the t test for dependent variables was used to verify differences in the 2 measurements obtained in each tooth. Significance level was set at 5%.
Results: Within a tolerance level of ± 0.5 mm, no significant differences were observed between the tested EALs regarding the absolute distance values (P = .82) or in their ability to detect the position of the major foramen (χ² = 0.2588; P = .6109). The accuracy of the Root ZX II and the Wirele-X apex locators within ± 0.5 mm were 81.8% and 90.9%, respectively.
Conclusions: Root ZX II and Wirele-X performed similarly regarding the in vivo detection of the major foramen. Using strict criteria, the accuracy of the Root ZX II and the Wirele-X apex locators were 81.8% and 90.9%, respectively. (J Endod 2022;48:1152–1160.)
Success or failure of endodontic treatment depends on the accurate determination of the working length (WL), which has been defined as the distance from a coronal reference point to the point at which canal preparation and filling should terminate. Historically, several methods have been used to determine the WL, such as radiographic examination and the patient response to pain, caused by passing of the instrument through the apical foramen. Undoubtably, the advent of electronic apex locators (EALs) provided an additional feature to the endodontic arsenal, overcoming the intrinsic disadvantages of the radiographic method, while reducing the treatment time and the radiation dose to the patient. Nowadays, a high level of precision and accuracy are important requirements of EALs to effectively determine the WL. Although precision (also reported as consistency, repeatability, reproducibility, or reliability) is how much subsequent determinations of the endpoint of the same canal with the same EAL differ from each other, accuracy is the ability of the EAL to locate the true endpoint of the canal. In an in vivo study in which the accuracy of 2 EALs in determining the WL in 482 canals was compared with the radiographic method, the authors concluded that all electronic measurements were within ± 0.5 mm of the minor foramen while, at this same range, radiographic exams were accurate in only 15% of the cases.
The recently launched Wirele-X apex locator (Forumtec, Ashkelon, Israel) is a wireless device that aims to extend the functional possibilities of EALs available on the market. According to the manufacturer, several new features were implemented in this EAL to ensure better precision and control (https://www.forumtec.net/products-apexlocators/). In contrast to other EALs that use mixed frequencies, measurements with the Wirele-X device are performed using alternating current signals at 2 alternated frequencies, cancelling the need for signal filtering and eliminating noise caused by nonideal filters. Moreover, the patented-based signal measuring method calculates the position of the file by the Root Mean Square and not signal amplitude or phase. This value represents the energy level of the signal and is more immune to various kinds of electromagnetic noises then other parameters of the measured signal. In addition, proprietary software algorithms are used to calculate the movement of the file in the root canal, offering a real time presentation of its position through a high-resolution color graphic display.
Many studies have pointed out the advantages, disadvantages, precision, and accuracy of different EALs. These assessments have been made both in vivo and in vitro and almost all of them used direct visual measurements of the distance from the file tip to some anatomic landmark at the apical canal by using scanning electron microscopy, stereomicroscopy, or radiography, with or without grinding the apical root. In other studies, the root structure was preserved and accuracy was determined by measuring the distance from the file tip to a silicone stop previously adjusted to the coronal surface of the tooth after determining the canal length by visualizing the tip of the file at the apical foramen. Although these methods have been successfully used for decades, none of them allowed for a detailed 3-dimensional (3D) analysis of the relationship between the tip of the file and the anatomic structures of the apical canal, an approach possible to be accomplished using high-resolution nondestructive micro-CT technology. In 2016, Piaseck et al used a micro-CT device to evaluate the accuracy of 2 EALs and concluded that the 0.5 mark could be used to properly determine the WL, whereas some anatomic variations of the root canal at the apical third could influence their accuracy.
Later, this same group used micro-CT to compare 3 EALs set at 0.0 and 0.5 marks in curved mesial canals of extracted mandibular molars and reported that Root ZX Mini (J Morita, Tokyo, Japan) and CanalPro (ColteneEndo, Cuyahoga Falls, OH) were precise in both marks, whereas the accuracy of Apex ID (SybronEndo, Glendora, CA) was higher at the 0.5 mark. In this same year, Connert et al used micro-CT to evaluate the accuracy of 9 EALs in 91 root canals by measuring the distances from the file tip to the apical constriction and major foramen. The authors concluded that using EALs to determine the major foramen led to an overestimation of the WL, recommending the use of EAL scale at the constriction level. More recently, Suguro et al compared the accuracy of 2 EALs in extracted teeth using micro-CT and reported that the apical foramen was located in 80% to 90% of the samples with a tolerance level of ± 0.5 mm.
Notwithstanding the successful application of a precise 3D analytical method to study the accuracy of EALs, the results of these studies clearly demonstrate that this topic is still embroiled in controversies.
Independent of the capability of an EAL to locate a certain morphologic landmark or area, the physiologic foramen (0.0 display mark) is the anatomic landmark that clinicians always attempt to determine at the first stages of the root canal treatment.
According to Piasecki et al, mean lengths obtained by using the 0.0 mark of the EAL are very close to the actual root canal length.
Considering the lack of literature information, the present study aimed to compare the in vivo accuracy of the Wirele-X and the benchmark RootZX II (J Morita) apex locators, set at the 0.0 display mark, in determining the position of the apical foramen in different teeth by comparing the electronic measurements with micro-CT images. The null hypothesis tested was that there is no difference between the Wirele-X and the RootZX II in determining the location of the apical foramen in an in vivo condition.
Material and methods
Sample Size Calculation
The minimal sample size for this study has been estimated using the G*Power 3.1 for Mac relying on a t test family for 2 dependent means. The effect size input (1.6) has been obtained from the results by Welk et al with an alpha error of 0.05 and power beta of 0.95. The results indicated a minimal sample size of 8 teeth to observe significant differences between the groups.
Sample Selection
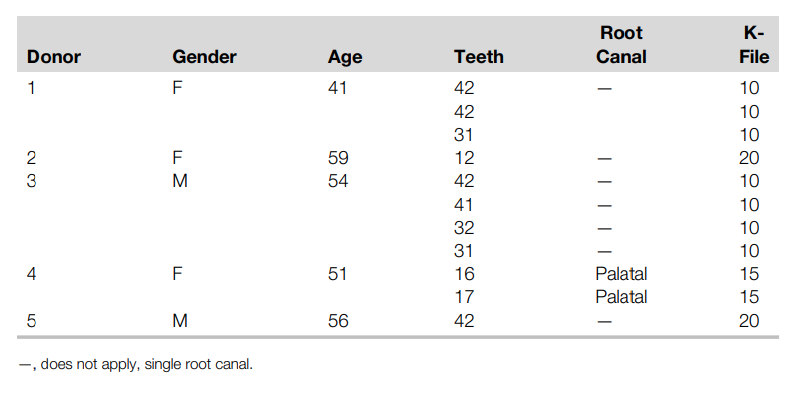
Five healthy adult patients referred for the extraction of 11 teeth due to periodontal or prosthodontic reasons participated in this study. Informed consent was obtained before treatment under a study protocol approved by the local research ethical committee (protocol 40352320.9.0000.5243). A preoperative periapical radiograph was taken using a digital sensor 5100 (Carestream Dental, Atlanta, GA) confirming that all experimental teeth had fully formed root apices, visible canals, no fracture, no resorption, no previous endodontic treatment, and adequate remaining tooth structure for rubber dam isolation. Pulp sensibility was assessed using Endo-Ice refrigerant spray (Hygenic Corp., Akron, OH) and recorded as either vital or necrotic after the pulp was accessed and vascular status determined. Only vital teeth were included in this study. The gender and age of the patients, the identification of the experimental teeth, and the selected canals of molars are depicted in Table 1.
Experimental Procedures
All teeth were treated under magnification by an operator with 15 years of clinical experience (V.B.C.F). After administration of local anaesthesia and isolation under rubber dam, existing caries and/or restorations were removed. The incisal edges and cusps were flattened with a cylindrical diamond bur using a high-speed handpiece under water irrigation to establish a level surface to serve as a stable reference for all measurements. After conventional access cavity preparation, the pulp chamber was irrigated with 2.5% sodium hypochlorite (NaOCl) for 1 min, and the coronal portion of the selected canal was flared using a Gates-Glidden drill size 2 (Dentsply Maillefer, Ballaigues, Switzerland). Then, the root canal was negotiated up to the apical third with sizes 08 and 10 K-files (Dentsply Maillefer), rinsed with 2.5% NaOCl, and the pulp chamber filled with the irrigant solution. Excess fluid was removed from the pulp chamber with cotton pellets and the WL of the canal was determined using 2 EALs: Root ZX II and Wirele-X. In each tooth, the order of EALs use was randomly assigned with a flip of a coin. The lip clip of the first selected EAL was then attached to the patient’s lip and a stainless-steel K-file was connected to the electrode of the apex locator. All of measurements were made with the first file to bind at the WL (Table 1). The file was gently inserted into the root canal until the numeric display of the apex locator reads “0.0.” This indicates the location of the major foramen according to the manufacturer’s instructions. All measurements were considered to be valid if the reading/signal on screen remained stable for at least 5 seconds. The silicon stop was then adjusted to the reference plateau created on the external surface of the crown. The WL was electronically rechecked to confirm the file position and the silicon stop was glued to the file with a synthetic adhesive composed of cyanoacrylate ester (Super Bonder, Henkel, Germany). After that, the file was withdrawn from the tooth, and a digital calliper (Mitutoyo, Tokyo, Japan) was used to measure the length between the tip of the instrument and the silicon stop to the nearest 0.01 mm. These procedures were repeated in the same canal with the second EAL using a different file with the same size. Teeth were then extracted and stored in distilled water.
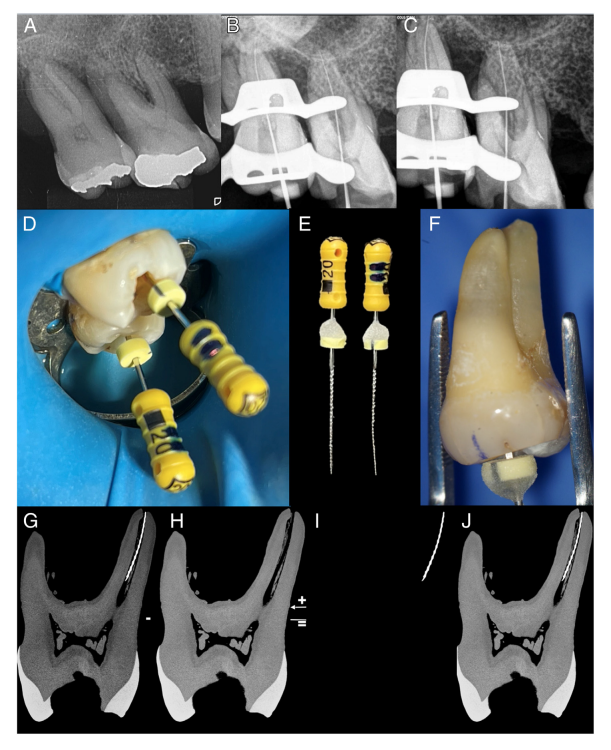
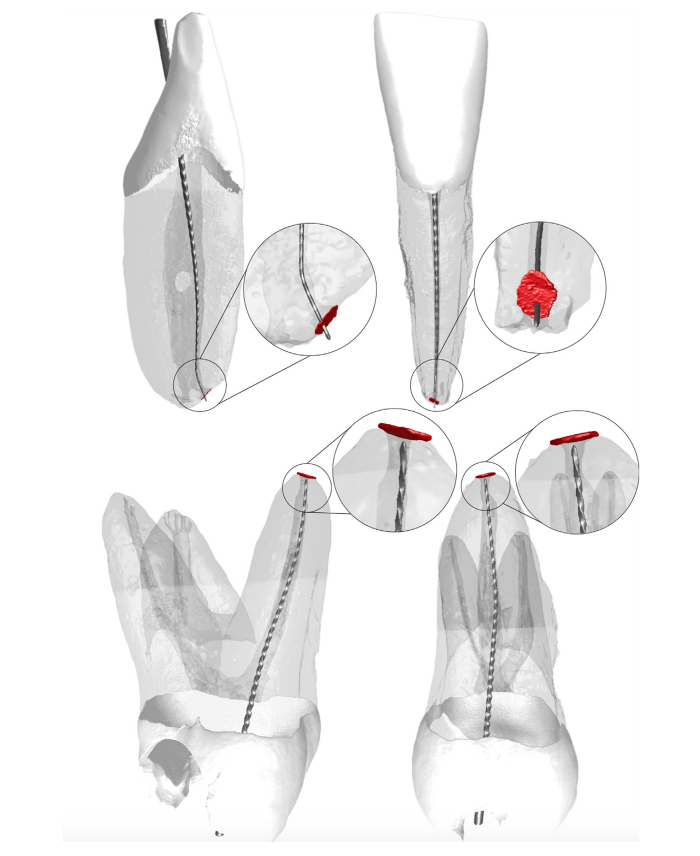
Micro-CT Scanning and Analyses Teeth were slightly dried and scanned in a micro-CT device (SkyScan 1173; Bruker-microCT, Kontich, Belgium) at a pixel size of 9.34 mm or 11.14 mm (according to the size of the tooth), frame average of 5, filtered with a 1.0-mm-thick aluminium plate, with (90 kV, 88 mA, 360˚ rotation with steps of 0.3˚) and without (70 kV, 114 mA, 360˚ rotation with steps of 0.5˚) the instrument inserted into the root canal space. Image reconstruction was performed using standard parameters for ring artifact correction (4) and beam hardening correction (40%), and contrast limits varied from 0.0 to 0.12 (with the instrument) and from 0.0 to 0.05 (without the instrument), resulting in 900 to 1200 grayscale cross-section images per tooth (NRecon v.1.7.16 software; Bruker-microCT). Then, image stacks without the instrument were co-registered to their respective datasets with the instrument within the root canal using the 3D Slicer 4.6.0 software (available at https://www.slicer.org/) aiming to visualize the dentin without the metal artifact created by the alloy. For each reading, the measurement error was calculated as the absolute difference, in millimeters, between the tip of the instrument and a tangent line crossing the margins of the major foramen (Figs. 1 and 2). Positive and negative values were recorded when the tip was detected beyond or short of the tangent line, respectively, using FIJI/ImageJ (Fiji v.1.51n; Fiji, Madison, WI) software. Accuracy was determined on stable measurements within ± 0.5 mm, excluding the ones extending beyond the apical foramen.
Statistical Analyses
The distances from the file tip to the tangent line were calculated for both groups and categorized in intervals of 0.05 mm into 4 groups. The frequency distribution of samples at each category was then calculated and the χ² test applied to verify differences between the tested EAL. The absolute distance values were also compared using a t test for dependent variables to verify the dissonances of the 2 measurements obtained in each tooth. Significance level was set at 5% (SPSS v.25; SPSS Inc., Chicago, IL).
Results
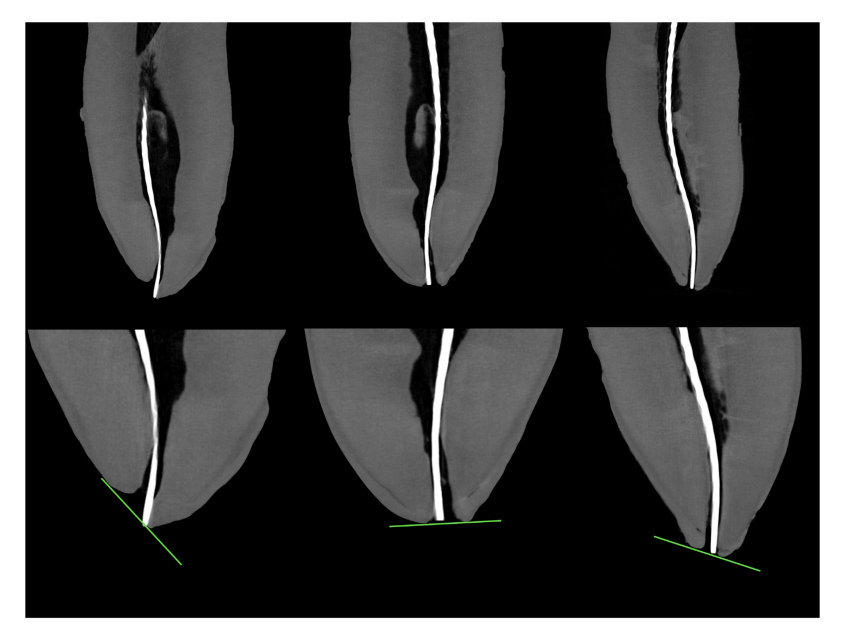
The frequency distributions of the distances measured by both EALs are depicted in Table 2. Within a tolerance level of ± 0.5 mm, no significant differences were observed between the tested EALs regarding the absolute distance values (P = .82) or in their ability to detect the position of the major foramen (χ² = 0.2588; P = .6109). The accuracy of the Root ZX II and the Wirele-X apex locators within ± 0.5 mm were 81.8% and 90.9%, respectively, excluding measurements obtained beyond the major foramen. Figure 3 illustrates the distances measured from the file tip to the tangent line in the selected canals.
Discussion
The present in vivo study was undertaken to compare the accuracy of a wireless apex locator (Wirele-X) with the well-known Root ZX II in detecting the position of the major foramen. This is the first research in which a wireless EAL was tested in patients and its accuracy was verified through the nondestructive micro-CT technology.
Consequently, our findings cannot be directly compared with the literature. Within a tolerance level of ± 0.5 mm, results showed no difference in the ability of Wirele-X and Root ZX II apex locators to detect the position of the major foramen (Table 2), and the null hypothesis was accepted.
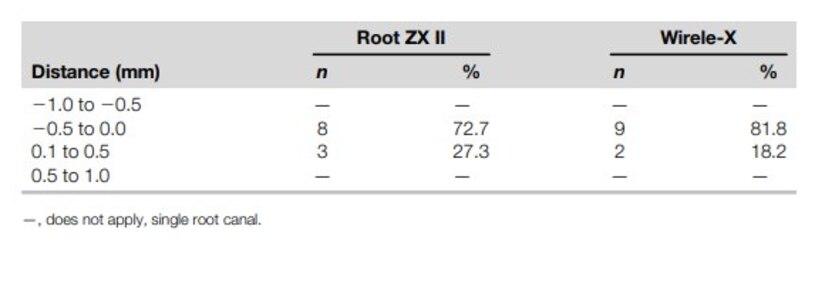
In this study, however, none of the tested EALs were able to precisely detect the position of the major foramen and, in 3 (27.2%) and 2 (18.2%) specimens of the Root ZX II and Wirele-X groups, respectively, the tips of the files were located outside the root canal space. These findings are corroborated by other authors that tested the Root ZX and reported the extension of the file tip beyond the major foramen in 40%, 32.1%, 30.8%, 26%, and 16.7% of the samples. Because of that, in the present study, when a strict clinical tolerance limit was applied, the obtained accuracies of the Root ZX II and the Wirele-X apex locators were 81.8% and 90.9%, respectively. These findings suggest that, in a clinical setup, WL determination with these EALs using the 0.0 mark would require an adjustment of the file to keep it within the limits of the root canal space.
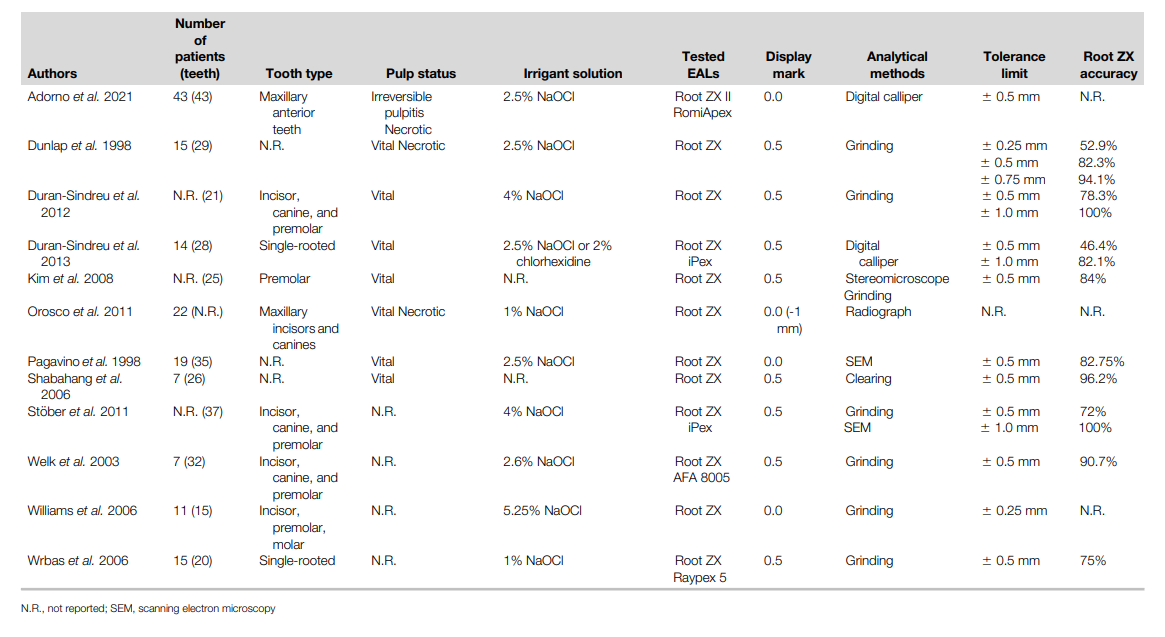
In the literature, several in vivo studies have tested the accuracy of the Root ZX in different groups of teeth (Table 3). In this type of study, electronic and/or radiographic WL determination is performed before tooth extraction and the confirmation of the actual WL is confirmed after extraction. Overall, when measurements are performed at the 0.5 display mark of the EALs, a wide range of accuracies were reported (46.4% to 99.8%) within ± 0.5 mm from the WL, possibly because of differences in the experimental conditions and methods of analysis. On the other hand, although some in vivo studies also used the 0.0 display mark as in the current research, only Pagavino et al reported the in vivo accuracy of the Root ZX (Table 3), which was similar (82.75%) to our findings (81.8%).
Some authors have suggested that the 0.0 and 0.5 display marks of the EALs can be used indistinctly because no statistical difference was observed in the WL determination with both of them. Although some manufacturers claim that these display marks locate the apical constriction and the major foramen, respectively, in fact they have been considered as arbitrary indicators of the more coronal or apical position of the file in the space between the apical constriction and apical foramen rather than of the exact location of these anatomic landmarks. This statement is supported by the present findings (Fig. 3) and also by Connert et al who compared the accuracy of 9 EALs in extracted teeth using micro-CT. Therefore, considering the limitation of EALs in locating the exact position of anatomic landmarks of the root canal, some authors suggested using the 0.0 display mark, as this allows for more accurate results.
In fact, the major foramen (0.0 display mark of the EAL) was chosen as the reference point in this study not only because its position can be consistently reproduced, rather than that of the minor foramen, but also because of the possibility of being easily identified in the acquired images. In addition, this study established the tolerance range at ± 0.5 mm from the apical foramen because this margin of error has been considered as an acceptable clinical limit of agreement for WL measurements made by EALs in most in vivo studies (Table 3).
In in vivo studies, destructive (grinding, clearing) and 2-dimensional (radiograph, calliper) methods have been the most commonly used procedures to evaluate the accuracy of the Root ZX after tooth extraction (Table 3). In the present study, micro-CT technology was chosen as the analytical tool because of the possibility of performing a 3D and nondestructive evaluation of the specimens. The double-scan protocol applied to the analysis allowed the reduction of artifacts produced by the alloy of instruments on dentin, enabling the precise location of the file tip position in relation to the apex (Fig. 1). Although micro-CT had been used to evaluate the electronic determination of WL in other studies, this is the first paper in which this methodological approach was applied to validate the accuracy of EALs after being used in patients. However, notwithstanding the clear advantages of micro-CT compared with conventional approaches, this type of study is costly and time-consuming. Besides, it is difficult to obtain a large number of similar teeth to conduct a series of measurements with different EALs and instrument sizes under different root canal environments because of economic and bioethical reasons, and this is one of the limitations of this study. On the other hand, attempts were made to reduce procedural errors by having the same operator assigning a random order to the EALs and performing the WL measurements in patients, while another operator, blinded to the used EAL, was responsible for conducting the analysis using micro-CT imaging.
In the past decades, technological advancements allowed the development of a large number of electronic gadgets aiming to improve the quality of root canal treatment. The EAL is possibly one of the most important devices of the endodontic armamentarium once it eliminates many of the problems associated with traditional radiographic methods. Throughout the years, EALs evolved from less accurate resistance-based apparatus to a new generation of precise multifrequency devices. The principle behind multiple-frequency EALs is based on the change in impedance of the file to tissue fluids. When the tip of the file is located away from the minor diameter of the canal, the impedance in the canal is negligible, but when the file reaches its vicinity, the magnitude of the impedance suddenly increases. As the file tip contacts the periapical tissue the impedance value rapidly decreases, indicating that the file is beyond the minor diameter of the canal. Whereas Root ZX II uses 2 different electric current frequencies (0.4 and 8 kHz), measurements with Wirele-X uses alternating current signals at 2 alternated frequencies. Although the manufacturer claims that its patented-based signal measuring method increases its precision by cancelling the need for signal filtering, as it eliminates noise caused by nonideal filters, no statistical difference was observed on its accuracy compared with the Root ZX II (Table 2).
The results of the present in vivo study confirm previous findings that demonstrate that EALs can accurately determine the canal length to within 0.5 mm from the major foramen (Table 3); however, in this study, only vital teeth were selected. Although some in vivo studies found no significant influence of pulp and periapical status on the accuracy of different EALs, they also reported larger standard deviation values and overestimated measurements in necrotic teeth. This is an important aspect to be considered mostly because laboratory and clinical reports also demonstrated that the disruption of the apical anatomy in necrotic cases might affect the accuracy of EALs. Therefore, it may be suggested that further in vivo and/or ex vivo studies aimed to compare the accuracy of recently launched wireless devices with conventional EALs and try to correlate the results with the diameter of the major foramen in teeth presenting different pulp and periapical status, using the methodological approach suggested herein.
Conclusions
Within the tolerance level of ± 0.5 mm, Root ZX II and Wirele-X performed similarly regarding the in vivo detection of the major foramen. Using strict criteria, the accuracy of the Root ZX II and the Wirele-X apex locators were 81.8% and 90.9%, respectively.
Authors: Gustavo De-Deus, Viviany Cozer, Erick Miranda Souza, Emmanuel João Nogueira Leal Silva, Ronald Wigler, Felipe Gonçalves Belladonna, Marco Simões-Carvalho and Marco Aurelio Versiani
References:
- Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: part 1: periapical health. Int Endod J 2011;44:583–609.
- AAE. Glossary of endodontics terms. 10th ed. Chicago: American Association of Endodontists; 2020.
- Gordon MPJ, Chandler NP. Electronic apex locators. Int Endod J 2004;37:425–37.
- Martins JN, Marques D, Mata A, et al. Clinical efficacy of electronic apex locators: systematic review. J Endod 2014;40:759–77.
- Adorno CG, Solaeche SM, Ferreira IE, et al. The influence of periapical lesions on the repeatability of two electronic apex locators in vivo. Clin Oral Investig 2021;25:5239–45.
- Vieyra JP, Acosta J, Mondaca JM. Comparison of working length determination with radiographs and two electronic apex locators. Int Endod J 2010;43:16–20.
- Pagavino G, Pace R, Baccetti T. A SEM study of in vivo accuracy of the Root ZX electronic apex locator. J Endod 1998;24:438–41.
- Kim E, Marmo M, Lee CY, et al. An in vivo comparison of working length determination by only root-ZX apex locator versus combining root-ZX apex locator with radiographs using a new impression technique. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105:e79–83.
- Pascon EA, Marrelli M, Congi O, et al. An in vivo comparison of working length determination of two frequency-based electronic apex locators. Int Endod J 2009;42:1026–31.
- Pascon EA, Marrelli M, Congi O, et al. An ex vivo comparison of working length determination by 3 electronic apex locators. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2009;108:e147–51.
- Piasecki L, Carneiro E, da Silva Neto UX, et al. The use of micro-computed tomography to determine the accuracy of 2 electronic apex locators and anatomic variations affecting their precision. J Endod 2016;42:1263–7.
- Piasecki L, Jose Dos Reis P, Jussiani EI, et al. A micro-computed tomographic evaluation of the accuracy of 3 electronic apex locators in curved canals of mandibular molars. J Endod 2018;44:1872–7.
- Connert T, Judenhofer MS, Hulber JM, et al. Evaluation of the accuracy of nine electronic apex locators by using Micro-CT. Int Endod J 2018;51:223–32.
- Suguro H, Nishihara A, Tamura T, et al. The use of micro-computed tomography to determine the accuracy of electronic working length with two apex locators. J Oral Sci 2021;63:167–9.
- Briseño-Marroquin B, Frajlich S, Goldberg F, et al. Influence of instrument size on the accuracy of different apex locators: an in vitro study. J Endod 2008;34:698–702.
- Welk AR, Baumgartner JC, Marshall JG. An in vivo comparison of two frequency-based electronic apex locators. J Endod 2003;29:497–500.
- Wrbas KT, Ziegler AA, Altenburger MJ, et al. In vivo comparison of working length determination with two electronic apex locators. Int Endod J 2007;40:133–8.
- Duran-Sindreu F, Gomes S, Stober E, et al. In vivo evaluation of the iPex and Root ZX electronic apex locators using various irrigants. Int Endod J 2013;46:769–74.
- Shabahang S, Goon WW, Gluskin AH. An in vivo evaluation of Root ZX electronic apex locator. J Endod 1996;22:616–8.
- Dunlap CA, Remeikis NA, BeGole EA, et al. An in vivo evaluation of an electronic apex locator that uses the ratio method in vital and necrotic canals. J Endod 1998;24:48–50.
- Stober EK, Duran-Sindreu F, Mercade M, et al. An evaluation of Root ZX and iPex apex locators: an in vivo study. J Endod 2011;37:608–10.
- Orosco FA, Bernardineli N, Garcia RB, et al. In vivo accuracy of conventional and digital radiographic methods in confirming root canal working length determination by Root ZX. J Appl Oral Sci 2012;20:522–5.
- Williams CB, Joyce AP, Roberts S. A comparison between in vivo radiographic working length determination and measurement after extraction. J Endod 2006;32:624–7.
- Jung IY, Yoon BH, Lee SJ. Comparison of the reliability of "0.5" and "APEX" mark measurements in two frequency-based electronic apex locators. J Endod 2011;37:49–52.
- Oliveira TN, Vivacqua-Gomes N, Bernardes RA, et al. Determination of the accuracy of 5 electronic apex locators in the function of different employment protocols. J Endod 2017;43:1663–7.
- Duran-Sindreu F, Stober E, Mercade M, et al. Comparison of in vivo and in vitro readings when testing the accuracy of the Root ZX apex locator. J Endod 2012;38:236–9.
- Jakobson SJ, Westphalen VP, da Silva Neto UX, et al. The accuracy in the control of the apical extent of rotary canal instrumentation using Root ZX II and ProTaper instruments: an in vivo study. J Endod 2008;34:1342–5.
- Lee SJ, Nam KC, Kim YJ, et al. Clinical accuracy of a new apex locator with an automatic compensation circuit. J Endod 2002;28:706–9.
- Stober EK, de Ribot J, Mercade M, et al. Evaluation of the Raypex 5 and the Mini Apex Locator: an in vivo study. J Endod 2011;37:1349–52.
- Kobayashi C, Suda H. New electronic canal measuring device based on the ratio method. J Endod 1994;20:111–4.
- Broon NJ, Palafox-Sanchez CA, Estrela C, et al. Analysis of electronic apex locators in human teeth diagnosed with apical periodontitis. Braz Dent J 2019;30:550–4.
- Piasecki L, Carneiro E, Fariniuk LF, et al. Accuracy of Root ZX II in locating foramen in teeth with apical periodontitis: an in vivo study. J Endod 2011;37:1213–6.
- Saatchi M, Aminozarbian MG, Hasheminia SM, et al. Influence of apical periodontitis on the accuracy of 3 electronic root canal length measurement devices: an in vivo study. J Endod 2014;40:355–9.
- Goldberg F, De Silvio AC, Manfre S, et al. In vitro measurement accuracy of an electronic apex locator in teeth with simulated apical root resorption. J Endod 2002;28:461–3.
- Stein TJ, Corcoran JF, Zillich RM. Influence of the major and minor foramen diameters on apical electronic probe measurements. J Endod 1990;16:520–2.