
Sagittal Condylar Angle and Gender Differences
Abstract
Purpose: The purpose of this study was to measure sagittal condylar inclination (SCI) in male and female participants and to assess differences between the two groups. This measurement has a clinical value in setting the articulator SCI before fabrication of indirect restorations.
Materials and Methods: The study included 32 dental students, 16 men and 16 women (aged 18 to 40 years). The participants had no signs of muscular or articular pain. SCI was recorded for participants using a CADIAXR compact 2 electronic axiograph.
Results: The mean SCI in both men and women varied between 26.1° and 61.8°, with a mean of 41.9° (SD 7.8). The mean right SCI was 42.0° (SD 8.5), and the mean left SCI was 41.9° (SD 9.2). The mean SCI for men was 40.3° (SD 7.9), and the mean for women was 43.6° (SD 7.7). No statistically significant difference in SCI values was found between the right and left side (p = 0.995), or between the male and female groups (p = 0.133). Also, no correlation could be found between SCI and the age of the participants (r2 = 0.016, p = 0.489).
Conclusions: The mean value of SCI was within the range reported in previous studies. SCI is highly variable, but this variability does not seem to be attributed to condylar asymmetry, gender, or age of the adult participants. This high variability suggests that independent condylar measurements should be conducted for each patient instead of relying on reported average values.
In restorative dentistry, an unplanned alteration of a patient’s existing occlusion should always be avoided to prevent tipping the existing balance in the patient’s masticatory system; however, in some situations the occlusion has to be reorganized due to esthetic or functional reasons. Occlusal reorganization in these situations should be planned very carefully to achieve the goals of ideal occlusion.
In patients where the anterior guidance is nonexistent and the posterior condylar guidance predominates, restorations should be made that do not interfere with the posterior condylar guidance. This can be achieved either by using average condylar values to set the articulator condylar mechanism or, more favorably, by recording and transferring the patient’s own condylar values.
Measurement of condylar movement in dentate adults has been the subject of intensive investigation by many researchers. In the sagittal plane, the inclination of the condylar path during protrusive movement is highly variable. Previous studies have reported values for sagittal condylar inclination (SCI) ranging from as low as 8° up to nearly 70°, with the mean value of most studies occurring between 30° and 45°.
SCI is traditionally measured by one of three methods: radiographic, intra-oral, or positional wax record, and graphical registration. These methods were then replaced by using more reliable pantographic measurement devices. Electronic axiography devices for TMJ movement recording were then developed to minimize errors associated with the transfer of information from a mechanical pantograph to a fully adjustable articulator and to improve efficiency by reducing the time involved in a pantographic procedure. Measurements of 3D condylar movements and articulator settings are obtained directly without the need to mechanically transfer the tracing to an articulator.
The purpose of this study was to measure SCI in male and female participants using an electronic axiograph. The null hypothesis tested is that there is no difference in the value of SCI between men and women. The results of this investigation can be considered by the clinician when selecting articulator type and setting the condylar mechanism of an articulator of male and female patients.
Materials and methods
Participants
Ethical approval for this study was obtained from the Committee on the Ethics of Research on Human Beings at the University of Manchester (ref: TPCS/ethics/09027). The sample size was calculated at a power of 80% for detecting SCI difference of a minimum of 5° at 5% significance level. To avoid sample bias, participants were mainly recruited through an e-mail advertisement forwarded to all undergraduate and postgraduate students via their respective administrators. Measurements were taken on 32 dental student volunteers (16 men, 16 women) from the School of Dentistry, The University of Manchester, with an age range of 18 to 40 years. Consent was obtained for each participant. All participants were dentate or with few missing teeth. Exclusion criteria were injury or disease of the skull or soft tissue structures of the skull or ears, extreme muscle pain in the head and neck region that makes wearing the pantograph and doing mandibular movements intolerable, dental and soft tissue problems that exclude mounting of a clutch, such as tooth mobility or loose restorations of the lower anterior and premolar teeth, and changes in the mucous membranes of the mouth, pronounced occlusal interferences, problems in the ear region such as ear inflammation, tinnitus, or pain.
Measurement of condylar movements
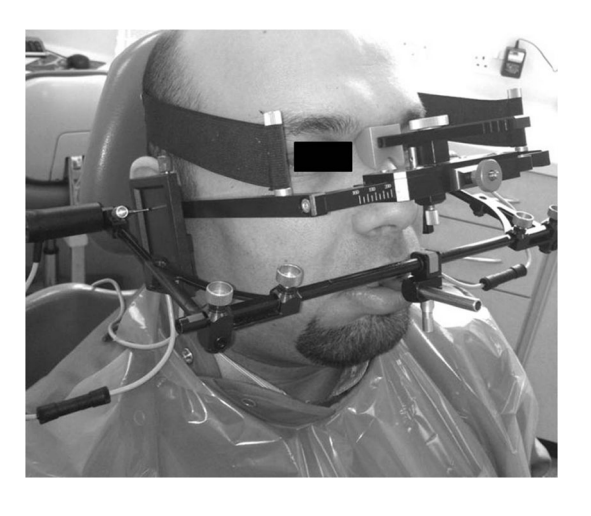
Condylar measurements were performed using a CADIAX compact 2 electronic axiograph (GAMMA Medizinischwissenschaftliche Fortbildungs-GmbH, Klosterneuburg, Austria). This system measures condylar movements in relation to the hinge axis-orbital plane. The transverse horizontal axis (THA) was arbitrarily located in relation to the external auditory meatus using a maxillary earbow.
To standardize the measuring procedure, all measurements were made by one trained operator. All measurements were made in the prosthodontics department at the University Dental Hospital of Manchester. TMJ and occlusal examination were carried out on each volunteer using Davies and Grey’s occlusal assessment guide. The CADIAX compact 2 for measuring mandibular movements was assembled and used according to the manufacturer’s instructions.
A sterile occlusal clutch was attached to the lower jaw at the anterior and premolar teeth area using silicone bite registration material with 43 shore hardness (Futar D, Kettenbach LP, Huntington Beach, CA). All recordings were made with the participant sitting in an upright position with the head supported (Fig 1).
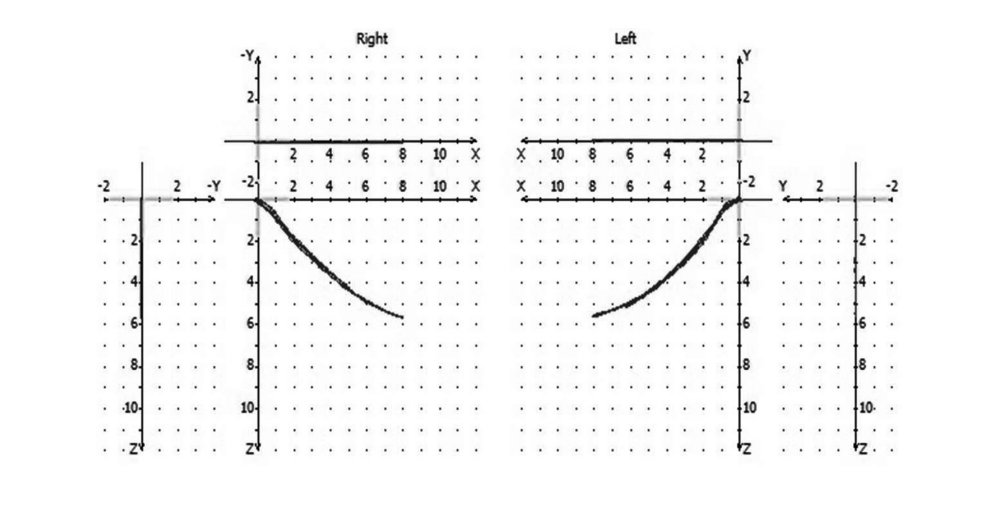
The reference point was set to the participant’s retruded contact position, which was obtained with operator chin guidance. After successfully determining the reference position, three protrusive mandibular movements were measured for each participant. The quality of each recorded curve was checked before starting the recording of the next movement. A good-quality record was achieved by making quick movements to the maximum distance that the mandible could go, and by avoiding any interference between the clutch and the upper teeth (Fig 2). Condylar inclination values in different planes and the corresponding suggested articulator setting values were obtained at the end of the recording procedure.
Three SCI values for both the right and left condyles of each participant were analyzed. The most consistent SCI values along the protrusive pathway were chosen. In most cases, these were the middle (fourth or fifth mm) SCI values. Data were entered into a statistical software package, (SPSS ver. 16.0; SPSS Inc., Chicago, IL) and checked for normality. Group differences were assessed with two-way ANOVA (side and gender as independent variables) at a significance level of p < 0.05.
Results
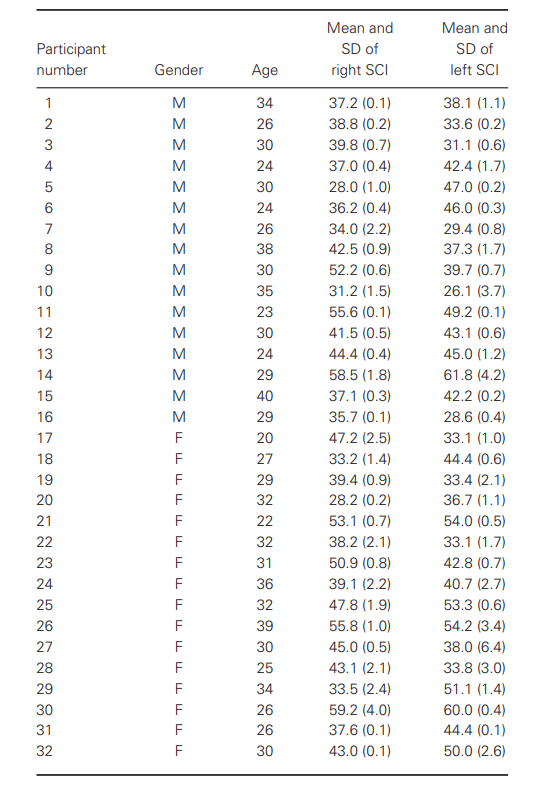
Data of recorded SCI are summarized in Table 1. SCI values varied between 26.1° and 61.8° with a mean of 41.9° (SD 7.8). In 66% of the participants, the mean SCI values ranged from 30° to 45°. The mean right SCI was 42.0° (SD 8.5), and the mean left SCI was 41.9◦ (SD 9.2). The difference between right and left SCI ranged from 0.5◦ to 19.0◦ with a mean difference of 6.7° (SD 4.6). In 84% of the participants, the difference between right and left SCI was less than 10.4°. There was no significant difference between the right and left SCI values (p = 0.995). The mean SCI for men was 40.3° (SD 7.9), and for women it was 43.6° (SD 7.7). There was no significant difference between male and female SCI values (p = 0.133). The mean age of participants was 29.5 years (SD 4.9). A simple linear regression analysis and a scatter plot were carried out to determine whether a relationship existed between age and SCI value. No clear pattern in the data or a linear relationship between age and SCI could be observed (r2 = 0.016, p = 0.489).
Discussion
Measuring technique
In this study, SCI was measured using a simplified computerized electronic axiograph, the CADIAXR Compact, which was first introduced in 1999. In vitro validity and reliability of this measuring system have been assessed using different preset articulators and testing the device in measuring different condylar inclinations, at different condylar track distances. The maximum measuring error for this system ranges from 0° to 3.4° with the smallest deviation related to SCI measurement at the tenth mm condylotrack distance, and increasing when the condylotrack distance decreases. This measuring error is considered clinically acceptable, at least in measuring SCI.
Comparisons of in vivo recordings of a Denar CADIAX compact with those of a Denar mechanical pantograph show that the CADIAX recordings lack consistency across time when compared to those obtained by the mechanical pantograph, especially those of the working pathways, which appeared irregular and short. That was explained by the relatively resilient silicone clutch relining material that can allow some clutch movement during recordings and was also attributed to the lack of central bearing point on the clutches of the CADIAX, which can make consistent reproduction of the centric relation reference point difficult to achieve. In 30% of the cases investigated by the CADIAX, the centric relation reference point was found to be reproduced inconsistently; however, that does not seem to affect the recordings of the protrusive or the nonworking pathways because of the much longer tracks of these condylar movements.
In this study, an ear maxillary facebow was used to practically locate an arbitrary hinge axis in relation to the external auditory meatus. A study showed that 75% of the axes located by an ear facebow fall within 6 mm of the true hinge axis. It has also been shown that an error of 5.0 mm in the location of the transverse hinge axis will produce a negligible anteroposterior mandibular displacement of approximately 0.2 mm when a 3.0 mm centric relation record is removed to close an articulator.
Accordingly, an ear facebow can be reliably used to locate an arbitrary hinge axis when a pantographic record is taken at a vertical dimension not altered to any significant extent.
SCI and its variability
The present study’s average SCI of 41.9◦ falls within the range of the reported values in previous studies. The closest results are those obtained by Payne and by Lundeen with a mean SCI of 42.7° and 45°, respectively. Based on the results of previous studies, it appears that SCI is highly variable. This variability can be related to true variability of SCI in the population, and can also be attributed to differences in measuring techniques. For example, the methods of graphic and pantographic registration may offer values different from those of intraoral wax based on the Christensen phenomenon where higher SCI values are obtained by the graphic method than by the wax method.
One factor in the measuring technique that can contribute to this variability is measuring SCI at different protrusive condylar track lengths. In most previous studies, the distance at which SCI was measured was not specified, and in some studies SCI value was the average value of the whole protrusive condylar track. This can result in variable SCI, because the condylar track is usually curvilinear as was classically reported by Aull in 1965. Thus SCI can vary considerably at different distances along the condylar track length. The SCI of the first 2 mm of protrusive condylar track is usually the most clinically relevant, because it is the distance at which the posterior teeth can be in contact during protrusive movement, before they get completely disoccluded by the anterior teeth guidance. In an in vitro investigation using the CADIAX compact, it was found that the standard deviation of the readings for SCI at 3 mm was twice as that for the readings at the tenth mm.
In a recent study on edentulous patients using the SAM electronic axiograph and a central bearing point, SCI was evaluated at 1, 2, and 5 mm of protrusion. The mean SCI was the lowest in the first mm (32.2◦) and it increased in the second mm to 40.4°, and increased further in the fifth mm to 44.5°. The fifth mm (41.94°), in which SCI was measured at the fourth or the fifth mean SCI in that study is very close to the result of this study mm, but the results might not be comparable due to differences in age and dental condition between the participants in these two studies.
Another factor that might contribute to variability in study results is the use of different horizontal reference planes. In most studies, the hinge axis-orbital plane was used, but in some studies other planes were used, such as the Frankfort plane and Camper’s plane. The Frankfort plane is represented by a line between the lowest points on the margin of the orbit anteriorly and the highest points on the margin of the auditory meatus posteriorly, while the hinge axis-orbital plane is represented posteriorly by the kinematic center of the right and left angle of about 13° to the horizontal plane while the Frankfort mandibular condyles. The hinge axis-orbital plane forms an plane forms an angle of about 8°. Camper’s plane is a plane running from the tip of the anterior nasal spine to the center of and it forms an angle of about 10° with the Frankfort plane the bony external auditory meatus on the right and left sides, These variations between the different planes make it apparent how inconsistency in SCI values can be obtained in different studies.
Right and left condylar variations
The results of SCI variations between the right and left sides are very close to those obtained by a previous study, which showed a mean of 36.6° and 37.7° on the right and left side, respectively. Similarly, in the majority of the participants in Posselt and Nevstedt’s study, the two condyles were asymmetrical, with 18 out of 101 participants having close to bilateral symmetry, and only one participant with full bilateral symmetry. Similar figures were also obtained in a more recent study on edentulous patients, where a range of difference of 0° to 25° between the right and the left side was found, with about 80% of the participants having bilateral asymmetry of less than 10°.
Gender differences
The mean SCI value for men was 40.3° (SD 7.9) and for women was 43.6° (SD 7.7), with no significant difference between the two groups at a 5% significance level. The same was found in previous studies, with similar mean SCI vales for male and female groups.
Variations related to age
The mean age of participants in this study was 29.5 years (SD 4.9). A scatter plot showed no clear pattern in the data or a linear relationship between age and SCI. The same was found by other studies with wider age ranges of 22 to 60 years and 15 to 63 years.
Conclusions
Within the limitations of this study the following can be concluded:
- The mean value of SCI of 41.9° (SD 7.8) falls within the range reported in previous studies.
- SCI is highly variable in the population.
- Variability in SCI does not seem to be attributed to condylar asymmetry, gender, or age differences of the adult participants evaluated in this study cohort.
- Large variations in reported SCI seem to be related to true variability, in addition to variability in measuring techniques.
The high variability of SCI suggests the need for carrying out independent condylar measurements for each patient instead of relying on reported average values, especially in extensive restorative cases where condylar guidance predominates and is significant. Condylar movement measurement using an electronic axiograph is considered a valuable tool that provides the information needed for deciding which type and setting of articulator should be used.
Authors: Ruwaida Z. Alshali, Riaz Yar, Craig Barclay & Julian D. Satterthwaite
References
- Davies S, Gray R: Occlusion: what is occlusion? Br Dent J 2001;191:235-245
- Posselt U, Nevstedt P: Registration of the condyle path inclination by intraoral wax records—its practical value. J Prosthet Dent 1961;11:43-47
- Gerber A, Steinhardt G: Dental Occlusion and the Temporomandibular Joint. Chicago, Quintessence, 1990
- Granger ER: The temporomandibular joint in prosthodontics. J Prosthet Dent 1960;10:239-242
- Ortman HR: The role of occlusion in preservation and prevention in complete denture prosthodontics. J Prosthet Dent 1971;25:121-138
- Johnson A, Winstanley R: Recording sagittal condylar angles using a mandibular facebow. J Oral Rehabil 1997;24:904-908
- Baqaien M, Al-Salti F, Muessig D: Changes in condylar path inclination during maximum protrusion between the ages of 6 and 12 years. J Oral Rehabil 2007;34:27-33
- Petrie CS, Woolsey GD, Williams K: Comparison of recordings obtained with computerized axiography and mechanical pantography at 2 time intervals. J Prosthodont 2003;12:102-110
- Curtis DA, Sorensen JA: Errors incurred in programming a fully adjustable articulator with a pantograph. J Prosthet Dent 1986;55:427-429
- Celar A, Tamaki K: Accuracy of recording horizontal condylar inclination and Bennett angle with the Cadiax compact . J Oral Rehabil 2002;29:1076-1081
- Chang WSW, Romberg E, Driscoll CF, et al: An in vitro evaluation of the reliability and validity of an electronic pantograph by testing with five different articulators. J Prosthet Dent 2004;92:83-89
- Teteruck WR, Lundeen HC: The accuracy of an ear face-bow. J Prosthet Dent 1966;16:1039-1046
- Weinberg LA: An evaluation of the face-bow mounting. J Prosthet Dent 1961;11:32-42
- Payne J: Condylar determinants in a patient population: electronic pantograph assessment. J Oral Rehabil 1997;24:157-163
- Lundeen H: Mandibular movement recordings and articulator adjustments simplified. Dent Clin North Am 1979;23:231-241
- Ecker G, Goodacre CJ, Dykema RW: A comparison of condylar control settings obtained from wax interocclusal records and simplified mandibular motion analyzers. J Prosthet Dent 1984;51:404-406
- Price R, Bannerman R: A comparison of articulator settings obtained by using an electronic pantograph and lateral interocclusal recordings. J Prosthet Dent 1988;60:159-164
- Aull AE: Condylar determinants of occlusal patterns. Part I: statistical report on condylar path variations. J Prosthet Dent 1965;15:826-846
- Hue O: Condylar Paths during protrusion in edentulous patients: analysis with electronic axiography. J Prosthodont 2011;20:294-298
- Pitchford JH: A reevaluation of the axis-orbital plane and the use of orbitale in a facebow transfer record. J Prosthet Dent 1991;66:349-355
- Olsson A, Posselt U: Relationship of various skull reference lines. J Prosthet Dent 1961;11:1045-1049
- Zamacona J, Otaduy E, Aranda E: Study of the sagittal condylar path in edentulous patients. J Prosthet Dent 1992;68:314-317
- Isaacson D: A clinical study of the condyle path. J Prosthet Dent 1959;9:927-935
- Beard C, Donaldson K, Clayton J: A comparison of articulator settings to age and sex. J Prosthet Dent 1986;56:551-554