
In Vivo Evaluation of Operative Torque Generated by Two Nickel-Titanium Rotary Instruments during Root Canal Preparation
Abstract
Objectives. This in vivo study evaluated the operative torque and preparation time of ProTaper NEXT (Dentsply Maillefer; Ballaigues, Switzerland) and EdgeFile X7 (EdgeEndo; Albuquerque, New Mexico, United States) rotary systems during root canal preparation of maxillary premolars.
Materials and Methods. Ten double-rooted maxillary premolars with independent canals were selected. Each canal in each tooth was prepared with one of the rotary systems (n = 10), ProTaper NEXT or EdgeFile X7. The instruments were rotated at 300 rpm with maximum torque set at 2 N.cm using an electric motor (KaVo; Biberach, Germany) that automatically recorded torque values at every 1/10th of a second (ds). Statistical Analysis Operative torque (N.cm) and preparation time (s) of the first shaping instrument (size 17/.04) of both rotary systems were recorded and statistically compared using the Mann–Whiney U test with a significance level set at 5%.
Results. No instrument exhibited flute deformation or underwent intracanal failure. No differences were found between the instruments regarding the maximum (peak) torque values (p > 0.05). EdgeFile X7 17/.04 required significantly less preparation time (3.75 seconds interquartile range [IQR]: 3.2–9.0) than ProTaper NEXT X1 (15.45 seconds IQR: 8.35–21.1) (p < 0.05). The median operative torque values of Pro- Taper NEXT X1 (0.26 N.cm; IQR: 0.18–0.49) were significantly higher compared with EdgeFile X7 17/.04 (0.09 N.cm; IQR: 0.05–0.17) (p < 0.05).
Conclusions. Although no difference was found between the median peak torque values of ProTaper NEXT X1 and EdgeFile X7 17/.04 instruments, the operative torque and instrumentation time results were impacted by their different designs and alloys during clinical preparation of root canals.
Introduction
Currently, many different brands of nickel-titanium (NiTi) rotary instruments are available in the market. Recent advances in metallurgy and manufacturing processes have allowed the development of instruments that are more flexible and resistant to fracture because of their innovative design and heat treatments.
It is obvious, that high-quality obturation begins with a well-prepared tooth. Mechanical instrumentation plays a pivotal role in endodontic success, ensuring precise cleaning, shaping, and sealing of the canal system. This meticulous process not only facilitates effective disinfection but also sets the stage for long-lasting restorative outcomes. We invite you to watch the lesson "Endodontics with NITI instruments" to ensure predictable outcomes in your endodontic cases!
ProTaper NEXT system (Dentsply Maillefer, Ballaigues, Switzerland) features a patented design that incorporates variable taper and off-centered rectangular core.
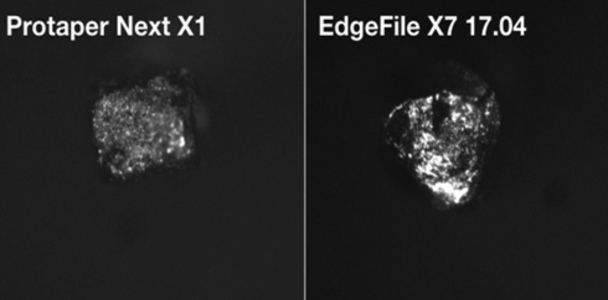
The instruments are made from M-Wire NiTi alloy, which enhances their flexibility and resistance to cyclic fatigue. According to the manufacturer, the axis of rotation of Pro- Taper NEXT differs from its center of mass. Thus, only two points of the rectangular cross-section contact the canal walls at time, potentially enhancing the shaping efficiency of the instruments. EdgeFile X7 instruments (Edge Endo; Albuquerque, New Mexico, United States) have a constant 0.04 taper, triangular cross-section, and variable helix angle. They are also manufactured by a proprietary process called FireWire, which is a combination of heat treatment and cryogenic applications that potentially not only increases the flexibility and resistance but also reduces the shape memory effect inherent of NiTi instruments (Fig. 1).
A previous study has shown that EdgeFile instruments had higher resistance to cyclic fatigue compared with Vortex Blue (Dentsply Sirona) and EndoSequence instruments (Brasseler USA, Savannah, Georgia, United States). Similarly, ProTaper NEXT has shown superior resistance to cyclic fatigue compared with ProTaper Universal (Dentsply Sirona) and Hyflex CM (Colténe Whaledent; Cuyahoga Falls, Ohio, United States). However, there is still limited data on the torsional resistance of these heat-treated NiTi rotary systems. Moreover, most laboratory tests usually provide only information about a single mechanical property at a time. On the contrary, many different factors can generate stress on the instruments during root canal preparation in clinics.
Recently, a new methodology was proposed to investigate the performance of rotary instrumentation in vivo by employing a dedicated software that records minimal variations in the torque, at short time-intervals, generated by an endodontic motor during root canal preparation. It was demonstrated that the torque required for Twisted-File (TF) rotary instruments (KerrEndo; Orange, California, United States) to reach the apical terminus of the canal, for example, was significantly reduced by previous coronal flaring. The torque of TF instruments was also impacted by the operative technique, being that an inward motion (or pecking motion) required more torque compared with the outward or brushing motion.
Considering that the high precision of this new operative torque measurement method could provide useful information regarding the clinical performance of different endodontic instruments, the present study aimed to compare the operative torque and preparation time of the first shaping instrument (size 17/.04) of ProTaper NEXT and EdgeFile X7 NiTi rotary systems, during root canal preparation of double-rooted maxillary premolars in vivo.
Materials and Methods
Ten patients (4 males, 6 females) aged 21 to 65 years old, (mean: 43.6 ± 12.42), with no contributory medical history, requiring root canal treatment of double-rooted maxillary premolars, were selected among those participating in a clinical research project on tooth anatomy based on cone beam computed tomography at the Dental Clinic of “Sapienza” University of Rome (Ethical Committee Protocol no. 528/17).
Informed consent was obtained from each patient before the experimental procedure. Following clinical and radiographic examination, only teeth presenting two roots and two independent canals, categorized as minimal or moderate difficulty according to the Assessment Form and Guidelines for Endodontic Case Difficulty of the American Association of Endodontists, were included. Exclusion criteria were teeth with anomalies, history of trauma, previous endodontic treatment, root resorption, nonpatent canals, severe canal curvatures (>30), canals larger than a size 20 K-file, or other canal configuration type.
In endodontics, the right access is the foundation of success. Properly designed access cavities ensure effective treatment planning and execution, especially when dealing with complex anatomical variations. Join the course "Access Cavity: Working with Complex Endodontic Anatomical Variations" and learn from renowned experts Dr. Gergely Benyőcs and Federico Foschi, who bring years of experience in managing challenging cases. Through detailed theoretical insights and practical demonstrations, this course will equip you with the skills to tackle even the most challenging endodontic cases, from access design to root obturation.
Conventional endodontic access cavities were prepared using round burs, following local anesthesia and rubber dam isolation. Irrigation was performed using 5% sodium hypochlorite and patency confirmed with a manual size 10 K-file. Working length (WL) was established using electronic apex locator (Apex ID; Kerr, Orange, California, United States) and a manual glide path was created in both buccal and palatal canals up to a size 15 K-file. One of the canals was randomly assigned for preparation with one of the two rotary systems: ProTaper NEXT or EdgeFile X7. The second canal of the same tooth was then prepared with the other system. Care was taken to ensure the same number of palatal and buccal canals in each group (n = 10).
All instruments were activated in rotary motion at 300 rpm with maximum torque set at 2 N.cm generated by a 1:1 contra-angle handpiece (KaVo, Biberach, Germany) powered by an electric motor (KaVo) (Fig. 2) with an inward (or pecking) motion (short amplitude and intermittent progression of the file 1 mm at a time) and slight apical pressure, up to the WL. This motor has a dedicated software that allows precise torque measurements of 0.01 N.cm automatically recorded in an incorporated memory card at every decisecond (ds), that is one-tenth of a second. In this study, only the torque values referred to the first instrument of each sequence were used for comparison because of their similar dimensions (size 17/.04). Additionally, preparation time during the inward movement of the 17/.04 instrument from the orifice up to the WL was recorded in seconds (s) with a digital chronometer.

Aiming to prevent bias related to operators’ skills, an experienced endodontist, previously trained in both rotary systems, performed all root canal treatments under magnification (4×) provided by an operating microscope. The files were cleaned at every 5 seconds of use to prevent debris accumulation in the flutes, during which root canals were irrigated with 3 mL of 5% sodium hypochlorite using disposable 28 G needle and plastic syringe. No lubricant paste was used.
New instruments were used to prepare each canal. After using the first NiTi rotary instrument, root canal preparation was completed according to the manufacturers’ guidelines using the sequential instruments of each system, but the torque data was not recorded because of the discrepancies in their dimensions.
After preparation, a final rinse with 3 mL 17% ethylenediaminetetraacetic acid for 5 minutes was performed in each canal. The canals were dried with paper points and obturated using warm vertical condensation technique. Access cavities were then restored using composite filling material (Sonic- Fill, Kerr, Bioggio, Switzerland).
All 17/.04 instruments were inspected under 10 × magnification for visible signs of deformation or fracture. Data of torque recorded in the memory card of the motor was exported as a digital spreadsheet document.
A power analysis for the variables of interest was based on a previous study to calculate the sample size (n = 10) with at least 80% of power to detect a significant difference in the mean torque values with α = 0.05. Data acquired during the experimental procedure was not normally distributed (Shapiro–Wilk test, p < 0.05) and results were statistically compared using the nonparametric Mann–Whitney U test using SPSS 20.0 Statistics (IBM Co., Armonk, New York, United States). Significance level was set at 5%.
Results
No instrument exhibited flute deformation or underwent intracanal failure. Table 1 shows the descriptive data (median and interquartile range) of peak torque and preparation time obtained after using ProTaper NEXT X1 and Edge- File X7 17/.04 rotary instruments for shaping root canals of maxillary premolars. EdgeFile X7 instrument reached the WL in significantly less time than ProTaper NEXT (p < 0.05). Root canal preparation with ProTaper NEXT X1 required a significantly higher median torque value compared with EdgeFile X7 17/.04 instrument (p < 0.05).
The maximum (peak) torque registered for EdgeFile X7 17/.04 instrument ranged from 0.04 to 2.0 N.cm, while for Pro- Taper NEXT X1 it ranged from 1.01 to 2.0 N.cm. However, no statistically significant difference (p > 0.05) was found between the tested instruments regarding the peak torque values.
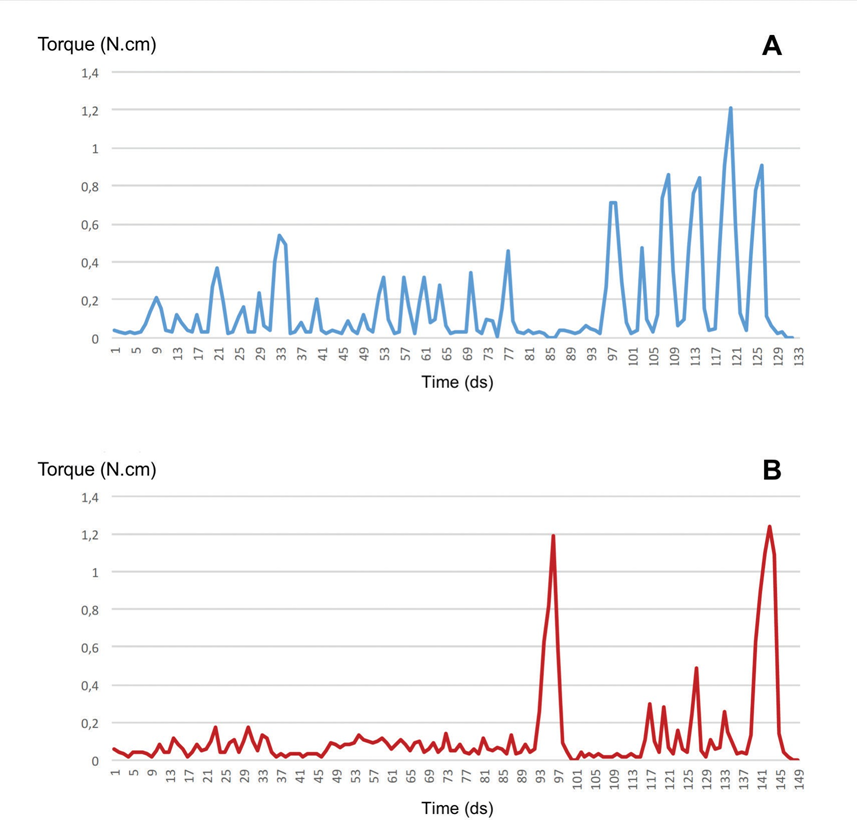
Figure 1 shows representative plots of the torque generated at concise time intervals (1/10 of a second) during clinical use of ProTaper NEXT X1 (Fig. 3A) and EdgeFile X7 17/.04 (Fig. 3B) instruments in each canal of a same tooth. The plots show the increase in torque over time which reflects the progression of the instrument from the canal orifice (time zero) to the WL, using inward movements of variable amplitude (wavelength), and regular stops for cleaning the flutes (flat spots).

Discussion
In the present study, a recently developed methodology was used to compare in vivo the operative torque generated by two different rotary systems during root canal preparation of the same tooth.
Operative torque of NiTi rotary instruments can vary depending on several factors including canal anatomy, dentin hardness, instrumentation technique, design and dimensions of the instruments, operator experience, and mechanical settings of speed and torque. Aiming to optimize comparison between instruments, care was taken in this study to minimize bias related to the anatomy and operator including the selection of same type of tooth (maxillary premolars) showing similar root and root canal morphologies. To prevent differences related to dentin hardness and calcifications (which can be age dependent), in each tooth, each canal was assigned to one of the tested systems.
It has been demonstrated that the smaller the canal dimensions, the higher is the torque needed to cut dentin, remove debris, and progress to the canal terminus. In a previous in vivo study employing the methodology used here- in, it was observed that the torque and preparation time during root canal preparation with TF 35/.04 instrument were significantly lower in canals previously flared coronally. Thus, in the present investigation, a manual glide path to a size 15 K-file was established without coronal preflaring. Consequently, the operative torque was measured from the beginning of the canal shaping procedure, without the influence of previous coronal enlargement.
Age of patients and hardness of dentin may influence the normality of torque values: the harder is the dentin, the more torque is needed to cut and progress inside the root canal. This explains why we used one instrument in the first canal and the other one in the second canal of the same tooth, to minimize the above-mentioned bias. Figs. 1 and 2 show the duration of instrumentation and peak torque values. In nearly all cases, the higher torque was generated in the apical third and torque values increased proportionally to the insertion (blade engagement) of the instrument. In a few cases, however, the torque recorded in the coronal part was higher than the torque recorded in the middle part. This could be related to a presence of some calcifications close to the orifice.
For both tested multifile rotary systems, 17/.04 instrument is recommended by the manufacturers in the first step of shaping procedures. Considering that the sequential instruments of these systems differ in their dimensions (size and taper), hampering comparison between them, in the present study operative torque was measured only for the first shaping instrument of each system, which presents equal nominal size and taper (17/.04), but noted differences in flute design and heat treatment. Such differences impacted the mean operative torque values, corroborating previous studies that correlated the design of the instruments to their performance. Rotary instruments with radial lands or wider cutting surfaces are more prone to contact a large surface area of the root canals walls, increasing its lateral resistance and, consequently, the torque generated during preparation procedures.
In this study, operator attempted to use the instrument until the WL using minimal apical pressure. Overall, the performance of both systems allowed to prepare the canals smoothly and torque limit settings were reached only in few canals. However, EdgeFile X7 17./04 instrument reached the WL with significantly less time and torque compared with ProTaper NEXT X1 (Table 1). Since all instruments were rotated using the same motor settings, this finding might be explained by differences in taper, cross-sectional design and characteristics of the alloy. Manufacturing process of NiTi rotary instruments may also influence in the generated torque during root canal preparation. Theoretically, a design that allows improved cutting efficiency should require less torque and also less time for root canal preparation. In the present study, results indicate that EdgeFile X7 17/.04 instruments were more effective in the preparation of root canals in vivo than ProTaper NEXT X1.
In this in vivo study, the recorded operative torque values were usually lower than the maximum set in the motor, in accordance with previous findings using the same methodology. The torque limit (2 N.cm) was reached only in few cases (two for EdgeFile X7 and three for ProTaper NEXT group) and no statistically significant difference was found between the two tested instruments regarding the peak torque values (Table 1). These results are in accordance with ISO 3630–1 specification, which revealed that torsional failure for a size 20/.04 rotary instrument was lower than 1 N.cm. Accordingly, no flute deformation or instrument separation could be observed. However, even if no difference was found regarding the peak torque values, the methodology was able to assess statistically significant differences in the mean operative torque values between the tested instruments, suggesting that recording only peak torque values would result in a partial analysis of the actual instrumentation torque. Thus, a dynamic analysis of torque throughout the instrumentation procedures might be a more reliable parameter, and the clinical relevance of these findings needs to be addressed.
In clinics, low torque values to rotate NiTi instruments during root canal preparation are preferable since high stress induced by dentin cutting has been reported to be the main cause of instrument fracture and development of dentinal cracks. However, torque generated during canal shaping reflects not only the energy endured by the NiTi instrument but also the stresses applied to the root dentin. Interestingly, the present results were lower than those reported in a laboratory study using a reciprocating heat-treated NiTi system (WaveOne Gold; Dentsply Sirona). Differences in the methodology (in vivo or ex vivo), kinematics and root canal morphology of the selected teeth could explain the divergence of the results. Additionally, since dentin properties are preserved in vivo and intracanal stress is detected by real operative torque, the present results can be considered more accurate compared with studies using extracted teeth.
Laboratory tests usually focus on evaluating a single parameter of the mechanical behavior of the instruments. However, in clinics, torsional, cyclic, and moderate bending stresses are simultaneously applied to the endodontic instruments during preparation procedures. In this in vivo study, for example, more than 100 torque and speed measurements were recorded in real time and plot in graphics for each root canal. Fig. 3 shows that it is possible to observe that during the progression of the instruments into the canal to the WL, both anatomical irregularities and pecking motion changed the engagement of the instrument against the canal walls, promoting variations in the generated torque. Lower torque values and shorter wavelength were observed in the first half of the plots, while instruments were enlarging the coronal and middle portions of the canal, reflecting their easiest progression as the amplitude and frequency of the inward motion is a function of the hindrance of the progression of the instrument into the canal. The detailed information provided by these plots can be useful in the analysis of the clinical performance of NiTi rotary instruments during preparation procedures. Consequently, this methodological approach can be considered much more reliable and of relevance to clinicians than laboratory tests, also because factors influencing torque like dentin humidity and intracanal pulp tissue are not changed by the extraction and\or storage process.
Even though the nominal size of the tested instruments was the same (17/.04), EdgeFile X7 has a constant taper, while ProTaper NEXT incorporates a variable regressive taper design, which results in a larger dimension of its coronal part. Consequently, engagement of the tested systems within the root canal walls was different. The initial progression of EdgeFile X7 instrument into the canal resulted in lower torque values and shorter amplitude pecking motion, with sudden increases (peak torque values) (Fig. 1B), which might be related to an engagement resultant of taper-lock. On the other hand, the design and variable taper of ProTaper NEXT resulted in greater engagement of the instrument, generating more torque during the entire procedure with gradual progression toward the end of the shaping procedure (Fig. 1A).
For most cases, the peak torque and greater amplitude of the pecking motion were observed in the last 4 to 5 seconds of the plots, which correspond to the apical third (Fig. 1). These findings are probably related to the increased difficulty of progressing the instruments into the narrowest region of the canal or to the taper-lock effect when the coronal part of the instrument becomes fully engaged, generating more stress. Despite operator proficiency has been considered an important factor for reducing failure of NiTi rotary instruments, present results indicate that even when the same clinician prepared the canals using the same movement, individual features of each instrument resulted in different patterns of manipulation and torque generation.
In the present study only the first instrument of each sequence was tested because, in a previous study, it was shown that the torsional stress applied on the following instruments is related to the clinical use and the characteristics of the first NiTi rotary instrument.4 Therefore, more variables could influence the intracanal clinical behavior of the instruments. Moreover, the main goal of the present study was to show whether differences in design and manufacturing process could significantly influence the operative torque, clinically. Obviously, differences in the tooth anatomy, age and hardness of dentin, and differences in dimensions and tapers of the NiTi rotary files could influence the operative torque values, but these variables did not affect the results of the comparative study we designed. Future research should consider using the operative clinical torque also for comparison among different instruments, techniques, sequences, and kinematics.
Within the limitations of this in vivo study, it may be concluded that differences in design and alloy of the tested instruments impacted the operative torque and time to prepare root canals of maxillary premolar.
Authors: Gianluca Gambarini, Massimo Galli, Marco Seracchiani, Dario Di Nardo, Marco A. Versiani, Lucila Piasecki, Luca Testarelli
References:
- Plotino G, Grande NM, Mercadé Bellido M, Testarelli L, Gambarini G. Influence of temperature on cyclic fatigue resistance of ProTaper Gold and ProTaper Universal Rotary files. J Endod 2017;43(2):200–202
- Testarelli L, Plotino G, Al-Sudani D, et al. Bending properties of a new nickel-titanium alloy with a lower percent by weight of nickel. J Endod 2011;37(9):1293–1295
- Pedullà E, Grande NM, Plotino G, Gambarini G, Rapisarda E. Influence of continuous or reciprocating motion on cyclic fatigue resistance of 4 different nickel-titanium rotary instruments. J Endod 2013;39(2):258–261
- Gambarini G, Plotino G, Piasecki L, Al-Sudani D, Testarelli L, Sannino G. Deformations and cyclic fatigue resistance of nickel-titanium instruments inside a sequence. Ann Stomatol (Roma) 2015;6(1):6–9
- Gao Y, Shotton V, Wilkinson K, Phillips G, Johnson WB. Effects of raw material and rotational speed on the cyclic fatigue of Pro- File Vortex rotary instruments. J Endod 2010;36(7):1205–1209
- Dentsply Sirona. ProTaper NEXT directions for use. Available at: http://www.dentsplymaillefer.com/product-category/glide- path-shaping/protaper-next. Accessed July 20th 2018
- EdgeEndo. EdgeFile X7 directions for use. Available at: https://edgeendo.com/wp-content/uploads/2015/08/DFU- EdgeFile-x7.pdf. Accessed July 20th 2018
- Dosanjh A, Paurazas S, Askar M. The effect of temperature on cyclic fatigue of nickel-titanium rotary endodontic instruments. J Endod 2017;43(5):823–826
- Elnaghy AM. Cyclic fatigue resistance of ProTaper Next nickel-titaniumrotaryfiles. Int Endod J 2014;47(11):1034–1039
- Nguyen HH, Fong H, Paranjpe A, Flake NM, Johnson JD, Peters OA. Evaluation of the resistance to cyclic fatigue among ProTaper Next, ProTaper Universal, and Vortex Blue rotary instruments. J Endod 2014;40(8):1190–1193
- Yared GM, Bou Dagher FE, Machtou P. Cyclic fatigue of ProFile rotary instruments after clinical use. Int Endod J 2000;33(3):204–207
- Lee W, Song M, Kim E, Lee H, Kim HC. A survey of experience-based preference of Nickel-Titanium rotary files and incidence of fracture among general dentists. Restor Dent Endod 2012;37(4):201–206
- Iqbal MK, Kohli MR, Kim JS. A retrospective clinical study of incidence of root canal instrument separation in an endodontics graduate program: a PennEndo database study. J Endod 2006;32(11):1048–1052
- Gambarini G, Piasecki L, Di Nardo D, et al. Incidence of defor- mation and fracture of Twisted File Adaptive instruments after repeated clinical use. J Oral Maxillofac Res 2016;7(4):e5
- Sattapan B, Nervo GJ, Palamara JE, Messer HH. Defects in rotary nickel-titanium files after clinical use. J Endod 2000;26(3):161–165
- Wu J, Lei G, Yan M, Yu Y, Yu J, Zhang G. Instrument separation analysis of multi-used ProTaper Universal rotary system during root canal therapy. J Endod 2011;37(6):758–763
- Gambarini G, Seracchiani M, Piasecki L, et al. Measurement of torque generated during intra-canal instrumentation in vivo. Int Endod J 2019; 52(5):737-745
- Gambarini G, Seracchiani M, Piasecki L, et al. The effect of a brushing motion inside a sequence; an in vivo study. Ann Stomatol (Roma) 2018;9:72–76
- Gambarini G, Tucci E, Bedini R, et al. The effect of brushing motion on the cyclic fatigue of rotary nickel titanium instruments. Ann Ist Super Sanita 2010;46(4):400–404
- Schneider SW. A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Pathol 1971;32(2):271–275
- Yared GM, Bou Dagher FE, Machtou P. Influence of rotational speed, torque and operator’s proficiency on ProFile failures. Int Endod J 2001;34(1):47–53
- Schrader C, Peters OA. Analysis of torque and force with differently tapered rotary endodontic instruments in vitro. J Endod 2005;31(2):120–123
- Blum JY, Machtou P, Micallef JP. Location of contact areas on rotary Profile instruments in relationship to the forces developed during mechanical preparation on extracted teeth. Int Endod J 1999;32(2):108–114
- Jamleh A, Komabayashi T, Ebihara A, et al. Root surface strain during canal shaping and its influence on apical microcrack development: a preliminary investigation. Int Endod J 2015;48(12):1103–1111
- Sattapan B, Palamara JE, Messer HH. Torque during canal instrumentation using rotary nickel-titanium files. J Endod 2000;26(3):156–160
- Baek SH, Lee CJ, Versluis A, Kim BM, Lee W, Kim HC. Comparison of torsional stiffness of nickel-titanium rotary files with different geometric characteristics. J Endod 2011;37(9):1283–1286
- Gambarini G, Testarelli L, Milana V, et al. Angular deflection of rotary nickel titanium files: a comparative study. Ann Ist Super Sanita 2009;45(4):423–426
- Boessler C, Paque F, Peters OA. The effect of electropolishing on torque and force during simulated root canal preparation with ProTaper shaping files. J Endod 2009;35(1):102–106
- Gambarini G, Giansiracusa Rubini A, Sannino G, et al. Cutting efficiency of nickel-titanium rotary and reciprocating instruments after prolonged use. Odontology 2016;104(1):77–81
- Gambarini G, Pompa G, Di Carlo S, De Luca M, Testarelli L. An initial investigation on torsional properties of nickel-titanium instruments produced with a new manufacturing method. Aust Endod J 2009;35(2):70–72
- Dane A, Capar ID, Arslan H, Akçay M, Uysal B. Effect of different torque settings on crack formation in root dentin. J Endod 2016;42(2):304–306
- Kim HC, Cheung GS, Lee CJ, Kim BM, Park JK, Kang SI. Comparison of forces generated during root canal shaping and residual stresses of three nickel-titanium rotary files by using a three-dimensional finite-element analysis. J Endod 2008;34(6):743–747
- Gambarini G. Cyclic fatigue of nickel-titanium rotary instruments after clinical use with low- and high-torque endodontic motors. J Endod 2001;27(12):772–774
- Kwak SW, Ha JH, Cheung GS, Kim HC, Kim SK. Effect of the glide path establishment on the torque generation to the files during instrumentation: an in vitro measurement. J Endod 2018;44(3):496–500
- Gambarini G, Testarelli L, Galli M, Tucci E, De Luca M. The effect of a new finishing process on the torsional resistance of twisted nickel-titanium rotary instruments. Minerva Stomatol 2010;59(7-8):401–406
- Yared G, Bou Dagher F, Kulkarni K. Influence of torque control motors and the operator’s proficiency on ProTaper failures. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2003;96(2):229–233