
Silver and Titanium Pins in Dentistry
Machine translation
Original article is written in RU language (link to read it) .
In dental practice, metal products are quite common. Metal pins can be made of titanium, silver, and less frequently from other metals. Today, silver pins are used less and less in dentistry, as they have a number of negative characteristics. Dentists prefer pins made from other materials.
More useful information on this topic can be found in the webinar Pin-based core build-ups and fiberglass pins: the relevance of the technique.
Silver Fillers
The idea of making pins from silver was first proposed in the 1930s, and these products were cones made of pure silver, used for canal obturation. Today, silver pins can rarely be found in a dentist's arsenal.

Figure 1. Preparation of the canal for a metal pin.
Material Composition
The silver used to make pins contains minor inclusions of other metals, about 0.1-0.2%, with copper and nickel being the most common impurities.
Advantages of silver pins:
- silver is a hard, rigid material;
- X-ray contrast.
- Disadvantages of silver pins:
- they have a weak bacteriostatic effect;
- due to the inability to adapt the material to the shape of the root canal, they have low obturation properties;
- the minor impurity of other metals can cause corrosion of the pins;
- the products formed during the corrosion of silver pins have a toxic effect on body tissues and can cause tissue damage;
- they cause discoloration of the tooth tissues.

Figure 2. Adhesive preparation.
Initially, silver was chosen as the material for making pins due to its oligodynamic effect, which implies an antibacterial influence of silver ions, attributed to their affinity for certain bacterial enzymes.
Years of research have proven the antibacterial effect of silver ions, but they have also shown the absence of spontaneous release. It has been clinically proven that pure silver does not have an irritating or toxic effect on the body's cells, nor on bacterial cells.
However, the prolonged presence of a silver pin in the root of a tooth, its extended contact with tissue fluid and body tissues contributes to the occurrence of corrosion. The corrosion process is accompanied by the release of silver sulfate, as well as some other compounds with a powerful toxic effect, which can trigger an inflammatory reaction from the surrounding tissues. This has led to the increasingly rare use of silver pins in the process of endodontic treatment, with many specialists completely abandoning their use.
The indication for the use of silver pins is relatively short root canals with a round cross-section, necessarily in combination with sealers, since the pin cannot adapt to the walls of the canal and does not adhere to the dentin. The use of silver pins is only possible in conjunction with root sealants.
In case of the need for retreatment of the canal, which is not uncommon after using this technique, a properly fitted silver pin can be extracted quite easily from the canal. However, there are situations where this manipulation is impossible.
Titanium Pins
Titanium and inexpensive alloys based on it are used as the material for creating pins.

Figure 3. Fitting of the metal pin.
Positive characteristics of titanium:
- high resistance to corrosion;
- chemical neutrality, absence of interaction with biological environments, no established phenomena of galvanosis;
- hypoallergenic, no proven cases of rejection or allergic reaction to titanium products;
- thanks to modern technological processes, pins of various sizes and configurations can be created from titanium;
- the dentist independently processes the titanium pin, giving it the required unique shape directly during the restoration of the tooth;
- titanium has an optimal combination of physical-mechanical and manipulative qualities;
- the intraradicular fragment of the titanium pin has a special patented configuration (a combination of cylindrical and conical sections with a special ratio of their lengths);
- titanium pins are passive, as they lack cutting threads, and have ring grooves with an inclined lateral surface – in the shape of a "Christmas tree";
- the shoulder – the supporting element of any anchor pin, which guarantees the unloading of the root canal, ensures the stability of the future structure to constant lateral loads during chewing;
- the crown part of all pins is equipped with clear retention points – ring grooves, which are necessary for reliable fixation of the restorative material;
- the use of a titanium pin reduces the load on the root during operation, serving as a preventive measure against root fracture;
- high reliability of pin retention in the seating bed formed according to all requirements;
- allow for an increased service life of restorations and orthopedic constructions fitted on pins;
- X-ray contrast.
Disadvantages of titanium pins
- correspond to the disadvantages of silver pins;
- are subject to corrosion in liquid environments.

Figure 4. Treatment using metal pins.
Structural elements of titanium pins
The following structural elements of the titanium pin are commonly identified:
- head,
- shoulder,
- tail.
The head is the crown part of the pin, which most often has the shape of a cone or cylinder, equipped with grooves – retention points – on the side surfaces. In some models of pins, additional notches are made on the heads, which gives them even more resemblance to natural teeth.
The design of the titanium post head is carefully thought out to increase the surface area, which significantly enhances the retention of composite material during the restoration of a tooth crown.
The supporting element of the titanium post is the shoulder, which serves to provide support for the tooth root on the dentin, helping to significantly increase the stability of the structure against lateral chewing forces.
The intraradicular part of the titanium post is the tail. It ensures reliable retention of the post structure in the root canal and allows for even distribution of chewing load on the root. The tail can have a smooth surface, and some models are equipped with ring grooves or a screw thread. The most popular shape of the tail is cylindrical or conical. However, the most optimal solution is to execute the intraradicular section of the post in the form of a combination of conical and cylindrical segments.
Indications for the use of titanium posts
- Minor volume of lost tooth tissue.
- To prevent the fracture of the wall of the devitalized tooth.
- If gentle treatment is necessary.
- Significant destruction of the crown with IROPZ values > 0.8, provided that:
- the gingival part of the tooth wall is preserved and protrudes above the edge of the gum by at least 3 mm;
- hard tissues are preserved at the level of the gum edge;
- destruction of the tooth wall below the gum edge, but not more than a quarter of the root length; in case of deeper destruction, extraction is recommended.
Contraindications for the use of post structures
- In case of canal obstruction.
- In the presence of signs of inflammation in the periodontal tissues.
- Short roots, excessive thinning of their walls.
- Against the background of atrophy of the bone substance of the alveolar process 3/4 of the root height or more.
- Root resorption of more than one quarter of the length.
- Destruction of any wall of the root by more than a quarter of the length.
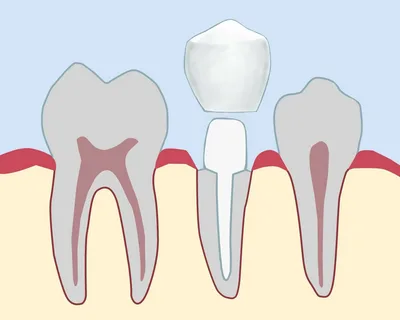
Figure 5. Diagram of the application of post structures in dentistry.
In the process of planning the manufacture of post structures, it is important to adhere to certain clinical conditions, primarily concerning the state of the root. The requirements for the tooth root necessary for the success of creating a post structure are:
- stability;
- the part of the root above the gum must be hard and show no signs of carious processes;
- strong walls (for lower incisors, a thickness of at least 1.0 mm, for other teeth – at least 2.0 mm);
- must be level with or above the edge of the gum;
- absence of curvatures along the first two-thirds of the length when viewed from the enamel-cement junction;
- the ratio of the length of the root to the height of the reconstructed crown cannot be less than 1.5:1.0;
- the apical third of the root canal must be properly filled, reliable obturation of the apical constriction is mandatory;
- absence of signs of inflammation in the periodontal tissues.
On the problems of intracanalar adhesion at the webinar Intracanalar Adhesion. How to Extend the Lifespan of Intracanalar Posts While Avoiding Adhesive Fixation Issues.