Errors in Endodontic Treatment at the Obturating Stage
Machine translation
Original article is written in RU language (link to read it) .
Despite the efforts of dentists and the constant improvement of endodontic techniques and protocols, failures can occur during treatment. Their number can be minimized, but it is impossible to completely eliminate them, as they are partly due to the physiological and anatomical features of the human body.
The selection of instruments for obturation is presented in the webinar Techniques for Working with Root Canals.
However, there are specific variable indicators that significantly influence the prognosis and success of treatment, and they depend on the professional experience and manual skills of the treating physician. Manipulations that lead to an unfavorable treatment outcome are considered "treatment errors." Any mistake increases the risk of complications, which may lead either to the need for retreatment or to the extraction of the tooth, and in some cases, may provoke a severe inflammatory disease.

Figure 1. Root canal filling.
This article will focus on the mistakes that can occur during the root canal filling stage.
The following types of errors in the root canal obturation stage are identified:
- Using only one paste for obturation that is prone to resorption in the canal.
- Fracture of the canal filler during the actual filling process.
- Fracture of the root in the longitudinal direction.
- Poor quality obturation.
- Filling material extruded beyond the root apex.
- Poor quality isolation of the root filling.
- Post-filling pain experienced by the patient.
Let's take a closer look at each of the aforementioned mistakes and discuss ways to eliminate them to prevent complications.
Using only a paste for obturation that is prone to resorption in the canal
The likelihood of resorption of the filling material used for root canal obturation significantly increases. In the future, this may lead to the formation of a focus of odontogenic chronic inflammation.
Preventive measures: following modern techniques for canal filling.
Elimination of consequences: performing repeated mechanical and medicinal treatment of the canal, followed by filling according to endodontic treatment standards.
Fracture of the canal filler during direct filling
Instrument fracture can occur against the background of insufficient processing and expansion of the canal, which provokes the jamming of the canal filler during its insertion into the canal and attempts at filling. Breakage can also be caused by a significant deviation of the canal filler from the axis of the root canal, which occurs due to leaving hanging edges in the canal or forming an incorrect endodontic access, or by accidentally winding a nearby cotton roll.
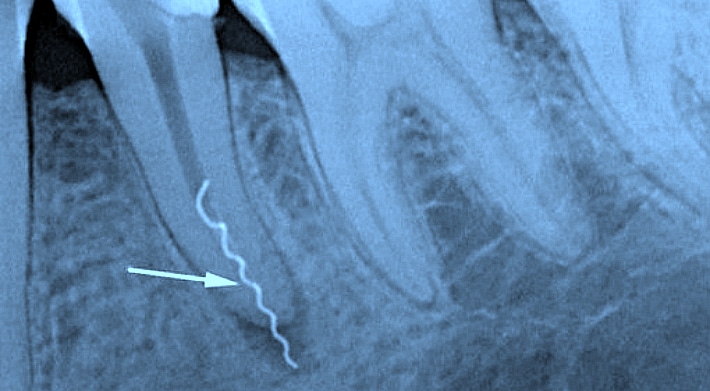
Figure 2. Fracture of the root filling in the canal.
Precautions: strict adherence to the rules for creating endodontic access to the tooth cavity, adequate and thorough mechanical preparation of the canal, compliance with the protocol, and careful manipulation with the root filling material, using low speeds when working with the root filling material (up to 500 revolutions per minute).
Removal: tool fractures are observed in the overwhelming majority of cases in the area where the shank transitions into the spiral, which allows for easy extraction of the fragment from the canal. If the fracture occurred in the area of the spiral itself and the broken fragment remains in the canal, it is not always possible to extract it. A more favorable situation arises if there is filling material alongside the spiral in the canal. It is necessary to perform radiological examination and assess the dynamics of the destruction focus in the apex area over a period of 4-6 months. If the possibility of extracting the canal filler is absent, conservative-surgical treatment techniques should be considered.
Root fracture in the longitudinal direction
The cause of the complication is excessive canal enlargement; application of force during the use of a spreader in lateral condensation of gutta-percha; careless work when preparing the canal for the anchor post. Clinical symptoms:
- the patient complains of pain when biting, touching the tooth;
- a crack is diagnosed in the area of the canal or at the bottom of the pulp chamber using a probe, which is easily identified using a caries marker; during visual inspection, the crack is sometimes soaked with fresh blood;
- slight mobility of the tooth fragments.
Precautionary measures: strict adherence to the protocol and careful work in the situations listed above. If a tooth fracture has occurred, it is not possible to eliminate this complication, and tooth extraction is required.
Poor Quality Filling
When evaluating the results of root canal filling, the presence of numerous voids, pores, and cracks indicates poor execution of the filling stage, which will lead to changes in the color of the tooth tissues in the future and the formation of a destructive form of periodontal inflammation.
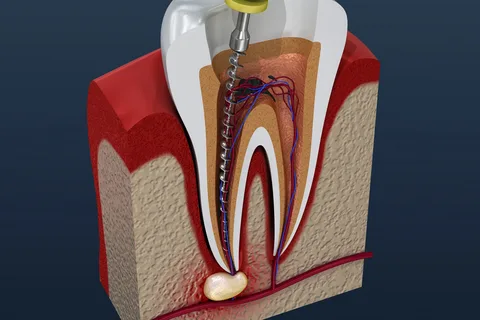
Figure 3. Pushing infected tissues beyond the apex.
Precautions: thorough mechanical preparation and medication treatment of the tooth canal, adherence to modern requirements for completed canal treatment (conicity of 6%, following the "irrigation protocol"), drying the canal before filling using paper points, and following all recommendations of the chosen canal obturation protocol.
Elimination of consequences: a poorly filled canal should be reopened, re-treated, and filled again.
Filling material extruded beyond the root apex
The material extruded beyond the apex causes mechanical irritation of the surrounding tissues, which will subsequently lead to the development of an inflammatory reaction. During the filling of the root canals of the molars of the lower jaw, the material, when extruded beyond the apex, ends up in the mandibular canal, provoking an inflammatory reaction of the mandibular nerve located there, which may result in permanent paresthesia. Due to the extrusion of material in the molars and second premolars of the upper jaw, the material may end up in the maxillary sinus, provoking inflammation of the latter.
Precautionary measures: determining the working length of the canal and strictly adhering to it when preparing the tooth for filling.

Figure 4. Extrusion of filling material beyond the apex.
Eliminating consequences: prescribing anti-inflammatory therapy; in some cases, physiotherapy has a positive effect. If such treatment does not show positive dynamics, the use of conservative-surgical techniques is considered, and in extreme cases, tooth extraction is indicated. If the patient is diagnosed with maxillary sinusitis, surgical treatment is necessary.
Poor Sealing of the Root Filling
The consequence of insufficient sealing of the root filling is micro-leakage, discoloration of the tooth, which is more pronounced in the cervical area.
Precautionary measures: when cutting gutta-percha pins with a hot instrument, it is necessary to minimize the shrinkage of the cooling gutta-percha by condensing it with a cold plugger or a thin burnisher; only after this is a complete sealing of the pulp chamber from the canal openings performed.
Elimination of consequences: removal of the crown filling, then if necessary, the canal is unsealed with subsequent reliable obturation, quality isolation of the material in the canal is performed, if indicated – whitening of the tooth tissues, the final stage is aesthetic restoration.
Occurrence of Post-Filling Pain in the Patient
Pain sensations in the patient can be observed even against the background of ideal canal filling, confirmed by radiological examination. The intensity of the pain component varies from mild tenderness when pressing on the tooth to an intense pain attack comparable to pulpitis pain.

Figure 5. Control of working length.
The following reasons for post-filling pain are possible:
- insufficient cleaning of the canal and penetration of infected tissues beyond the apex;
- use of materials that cause irritation, allergies, and neurotoxic disorders of the periapical tissues;
- trauma to the periapical tissues during canal treatment;
- premature obturation of the canal against the background of unresolved exudation processes during periodontitis;
- overfilling of the tooth.
Precautionary measures: strict adherence to the protocol at all stages of endodontic treatment.
Elimination of consequences depends on the cause of the complication: some patients require anti-inflammatory or desensitizing therapy, re-filling of the canal, correction of the filling, apex resection.
New protocols for root canal obturation are presented in the online course What’s NEW in Endodontics: from Anesthesia to Obturation.