
Pathological Erasability: Causes and Mechanisms
Machine translation
Original article is written in RU language (link to read it) .
Throughout life, chewing is accompanied by direct contact of opposing teeth, which results in the gradual loss of hard tissue on the occlusal surfaces of the tooth.
About the types and methods of diagnosing pathological wear at the webinar Pathological Wear. Classification. Diagnosis.
Hard tissues wear out in both temporary and permanent occlusions. The following types of tooth wear are distinguished:
- physiological,
- pathological.
The type is determined by the degree of severity of the process in a specific patient.
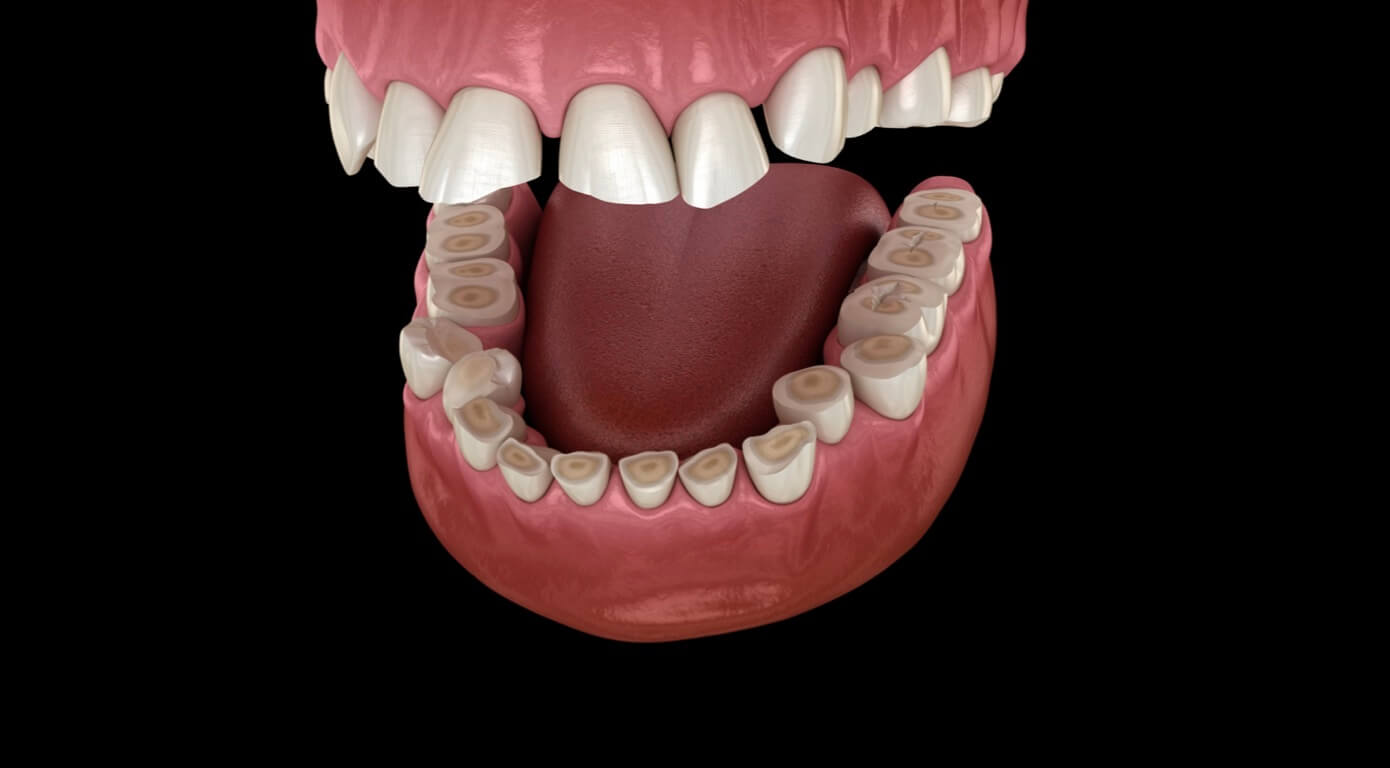
Figure 1. Pathological wear of teeth.
Physiological wear is an adaptive mechanism that protects the teeth from functional overload. It is a compensated, slow process that optimizes chewing function and ensures freedom of movement of the lower jaw, preventing obstacles to the smooth movement of the dental rows in any phase of articulation. Clinically, physiological wear involves the loss of tooth tissue within the enamel on the occlusal surface.
Pathological wear is a relatively fast-progressing process of tooth tissue loss (wear is not limited to enamel, dentin is also involved), which is accompanied by disturbances not only of the dental tissues but also of the surrounding tissues, characterized by changes in the temporomandibular joint and masticatory muscles.
Often, it is impossible to assess the difference between these two processes, which is the reason for difficulties in conducting differential diagnosis and planning treatment. The most objective way to assess the loss of hard tissues is by considering the patient's age.
Etiology
Increased tooth wear is considered a polyetiological disease. The variety of etiological factors causing wear can be divided into the following groups:
Functional insufficiency of tooth tissues. Caused by anatomical inadequacy, immaturity of enamel and dentin. In turn, it is divided into:
- hereditary (Stenton-Capdepon syndrome);
- congenital (pathology of amelo- or dentinogenesis due to diseases of the mother or fetus);
- acquired (resulting from neurodystrophic mechanisms, disorders of the circulatory and endocrine systems, and metabolic disturbances).
Excessive functional load on teeth, develops under the influence of the following factors:
- increased load on the remaining teeth after partial loss;
- presence of parafunctions in the patient (bruxism);
- chewing muscles are in constant hypertonus, which may have a central origin, or may be related to occupational hazards (physical stress, vibration);
- chronic trauma to the teeth, which also includes harmful habits of the patient;
- occlusal anomalies.
Occupational hazards (dust, exposure to alkalis and acids). Wearability may be related to the patient's illnesses – bulimia, achylia, for which the patient is prescribed hydrochloric acid intake. Early symptoms of pathological wearability are often associated with the habit of consuming certain foods that have an acidic effect – carbonated drinks.
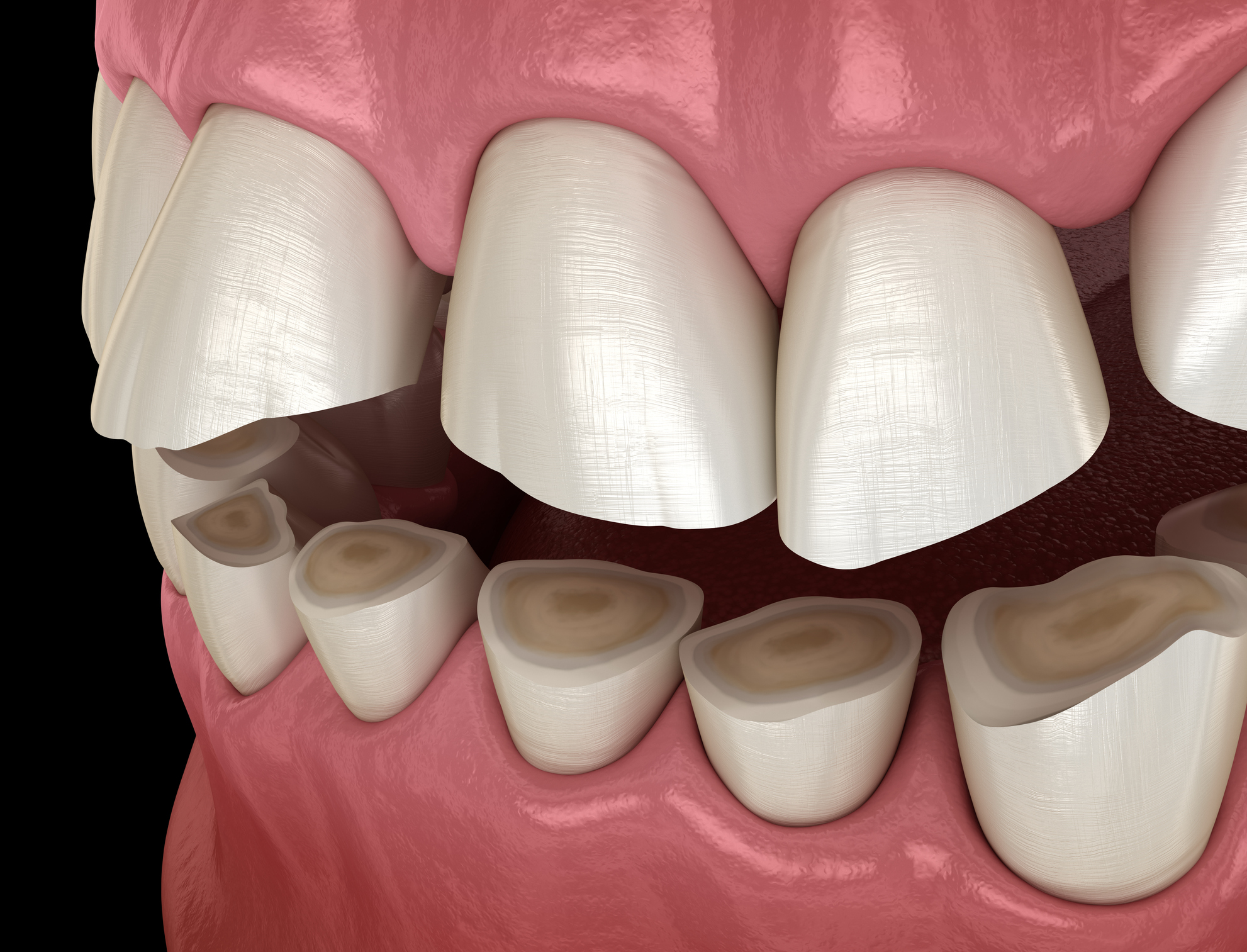
Figure 2. Wearability of tooth tissues.
It is also worth mentioning another group of factors — the increased abrasive impact of some materials on tooth tissues. Examples:
- constant consumption of hard food (frozen raw meat and fish among the Nenets);
- daily use of tooth powder, hard brushes over a long period of time;
- irrational selection of materials for denture and restoration of teeth.
Features of material selection
Today, clinicians have a wide range of materials available for the elimination of dental rows and the restoration of individual teeth, which provides an extensive list of alternatives in the treatment process, but at the same time complicates the choice of material that is most optimally suited in a specific clinical situation by the required characteristics.
Increased attention is paid today to biological compatibility, aesthetic indicators, costliness, and material strength. However, it is very important to consider the microhardness of the material, its value should approximate that of tooth tissues. This will help optimize the wear of the occlusal surface, achieve more uniform wear of the tooth tissues and the material of the prosthesis or restoration directly.

Figure 3. Wear within the dentin.
The next important criterion is the coefficient of friction between the selected material and tooth enamel. It is determined by the nature and characteristics of the rubbing surfaces, their roughness, the presence of lubrication, and the applied load. For example, plastic significantly lacks the microhardness compared to tooth enamel, but the abrasive impact of plastic is considerably greater. For this reason, it is not advisable to use plastic on one jaw and a gold alloy on the antagonist teeth in prosthetics, as this choice will provoke rapid wear of the latter.
Using ceramic prostheses on both dental arches on opposing teeth will slow down tooth wear, but may provoke an overload of the periodontium, as well as cause pathological changes in the temporomandibular joint. The aforementioned combination of materials should be used with caution; it is better to choose a porcelain-metal combination: install a bridge prosthesis made of metal on the upper jaw, this will not cause aesthetic disturbances, but will approximate the level of wear to the natural level for tooth enamel.
Today, manufacturers' developments are aimed at obtaining porcelain masses with lower hardness. This has already led to the release of a new variety of dental ceramics — low-fusing. The microhardness of this material is close to that of enamel. Such material virtually has no negative impact on the enamel of opposing teeth and is the material of choice for prosthetics in any clinical situation.
An insufficiently smooth surface of a ceramic structure can lead to iatrogenic wear; roughness appears due to a poor glazing stage, as well as the absence of re-glazing after adjusting the occlusal surface of the finished product. Instead of re-glazing, it is permissible to polish the adjusted fragments of the finished product using special polishes, which allow achieving a satisfactory level of smoothness for ceramic prostheses.

Figure 4. Crown made of gold alloy.
One should not forget about the pronounced abrasive effect of composite restoration materials, predominantly referring to macro-filled composites. Under the influence of chewing load, the surface areas of the matrix of these materials wear out rapidly, exposing the micro-particles of the filler, which are significantly hard and have a high friction coefficient. These material characteristics cause increased wear of the enamel of opposing teeth. For this reason, despite their good mechanical strength, the use of these materials in areas of high occlusal load is not recommended.
The polishing stage of restorations is not only an opportunity to achieve significant aesthetic results but also a preventive measure to prevent increased wearability.
The optimal solution for restoring the occlusal surface of posterior teeth is restorations made from silver amalgam, as well as prostheses made from noble metal alloys. However, with the increase in aesthetic demands of patients, these materials have been replaced by ceramic inlays made from modern ceramic masses.
Pathological tooth wear due to bruxism is caused by increased stress on the teeth. Experimental studies have shown that saliva is an effective lubricant, which is quite sufficient under normal load, but it is not enough to prevent increased wear under high load.
Pathogenesis
The changes observed in the tooth itself and the surrounding tissues do not depend on the cause of the disturbances of the chewing surface. There is a layering of replacement dentin, gradually there is obliteration of the tooth cavity and root canals. On the tooth section, the curvature and narrowing of the tubules, obliteration of the tubules, and calcification of these areas are clearly visible.

Figure 5. Uneven wear of hard dental tissues.
In the pulp, dystrophic disturbances are noted: the number of blood vessels decreases, they become sclerotic, the main substance undergoes hyalinization, calcium salts are chaotically deposited, dentin tubercles are formed, the layer of odontoblasts undergoes vacuolization, the pulp atrophies, and nerve fibers undergo degenerative transformations.
Classic orthopedic and composite protocols in the therapy of pathological wear in the online course Pathological Wear: Treatment.