
Hereditary disorders of tooth tissue structure
Machine translation
Original article is written in RU language (link to read it) .
Often, non-carious lesions of tooth tissue develop not as a result of external influences or systemic diseases, but are the result of a hereditary factor. The development of enamel is disrupted due to pathological changes that ectodermal cell formations undergo, resulting in an atypical structure of the dentin.
Amelogenesis imperfecta can be a cause of internal staining, learn more about this in the webinar Review of tooth whitening techniques: laser whitening, light whitening, home and office whitening.
The following types of hereditary tooth lesions are distinguished:
- amelogenesis imperfecta;
- dentinogenesis imperfecta;
- Stenton-Kapdepon syndrome;
- incomplete odontogenesis;
- marble disease;
- hypophosphatasia.
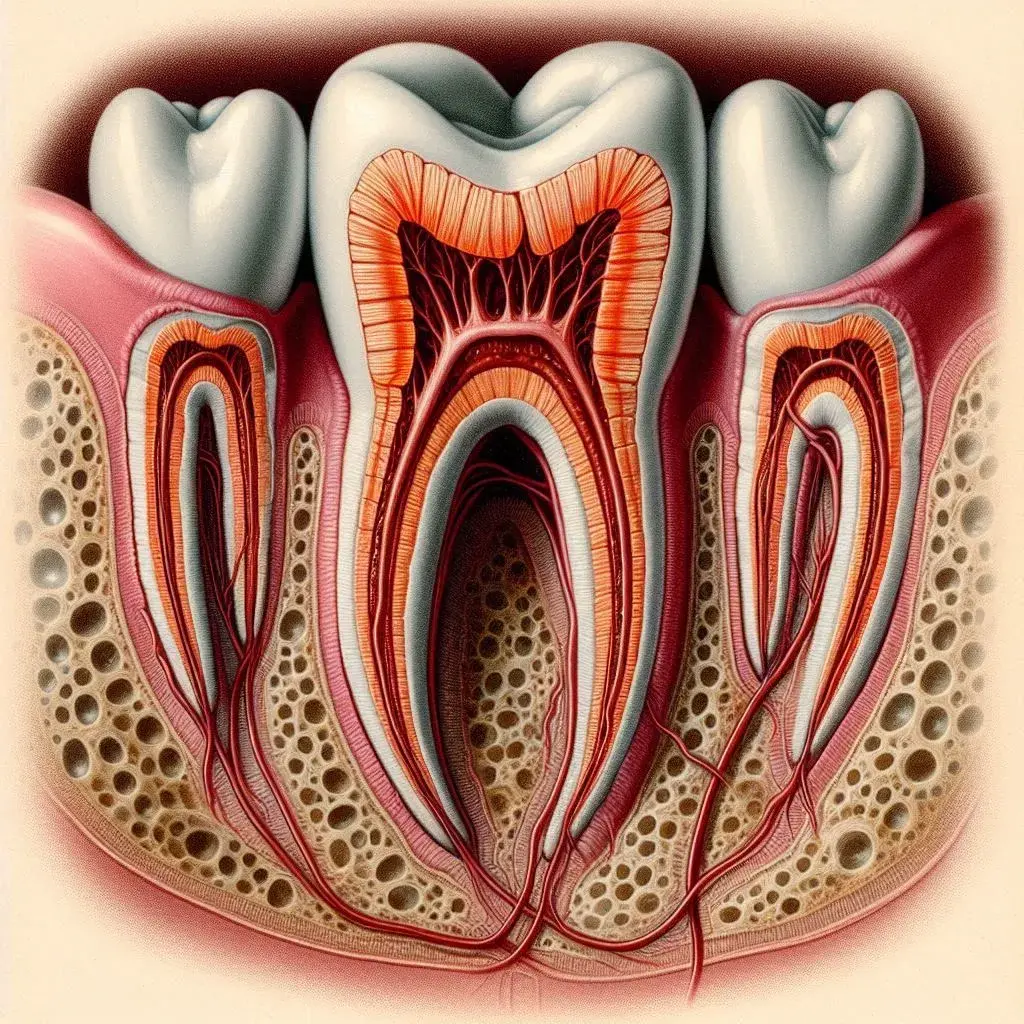
Figure 1. Normal structure of tooth tissues.
Incomplete Amelogenesis
This is a hereditary condition characterized by the pathological development of enamel. The clinical picture is determined by qualitative and quantitative enamel defects. Several types of incomplete amelogenesis are recognized.
- In the first type, there are few, often minor, enamel defects. It occurs with equal frequency among representatives of both sexes. These are practically healthy patients whose teeth erupt on time, but typically have smaller crown sizes. Due to the reduced width of the crowns, gaps appear between the teeth. The enamel retains its shine and smoothness but acquires a yellowish or brownish tint. Different areas of the same tooth may be colored in different shades. The tooth root has a normal configuration and length. The tooth cavity and canal lumens are clearly visible on an X-ray.
- The second type of hereditary enamel defect is characterized by more significant quantitative and qualitative transformations. This pathology occurs with equal frequency among representatives of both sexes. Teeth erupt on time, but the crowns are wider at the necks or uniform in width throughout; in the first case, the crowns are conical, and in the second, cylindrical. The tooth surface is rough because the enamel appears in the form of separate islands, predominantly in the cervical area. The teeth are colored in yellow and brown shades. The vestibular surface is more affected relative to the oral surface. The pathology is associated with structural enamel defects and weak mineralization. The dentin has a normal structure. The roots are of normal configuration and size, and the tooth cavity and canal lumens are clearly traced on an X-ray. Increased sensitivity to certain irritants, often temperature and mechanical, may occur. The crowns on the X-ray have uneven contours, due to the absence of enamel in these areas.
- In the third type of incomplete amelogenesis, teeth have normal sizes, shapes, and colors, but in some cases, the enamel is thinned and its shade is altered. However, in both cases, the tooth surface is marked with grooves that give the enamel a ridged appearance. Unlike systemic hypoplasia, these grooves are vertical, not horizontal. All teeth are affected, both deciduous and permanent. The grooves are localized across the entire crown surface. On the X-ray, the configuration of the roots, the lumen of the tooth cavity, and the canals are clearly traced. On the crowns, stripes of varying density, length, and width are identified, directed from the cutting edge to the neck.
- In the fourth type of crown damage, the crowns are of normal size, have the correct shape, but the enamel loses its shine, becoming chalk-like. Scientists believe this is due to the absence of the cuticle and pellicle—typical organic coatings for enamel. The enamel is unable to withstand mechanical impact and delaminates from the dentin at the slightest trauma. The exposed dentin is initially yellow, then acquires a brown coloration due to pigment penetration. As the enamel wears and chips, the size and configuration of the crowns change. Increased sensitivity of the exposed dentin to thermal irritants is observed.

Figure 2. Enamel hypoplasia.
The pulp's electrical excitability is normal. The shape of the roots, the tooth cavity, and the canal lumens are also within normal limits, only on the approximal surfaces are there translucencies resembling carious cavities, which correspond to areas with lost enamel.
Incomplete Dentinogenesis
It represents a hereditary pathology of dentin development, characteristic of individuals of both sexes.
Typical clinical manifestations
- Normal size, color, and shape of tooth crowns.
- Such teeth are rarely susceptible to caries.
- Common complaint of pain from thermal irritants.
- Patients often suffer from periodontal diseases, ranging from catarrhal gingivitis to mobility of teeth (predominantly front teeth) in the absence of periodontal pockets.
- The number of mobile teeth increases with age, individual teeth fall out.
- The roots are shortened, the tips are pointed. In multi-rooted teeth, the furcation area is located further from the tooth neck, with pointed projections identified at the root tips.
- The canal lumen is often not visible. Narrowing of the tooth cavity and canal lumen is a developmental defect of the tooth.
- At the root tips, areas of bone tissue rarefaction are noted, and with age, such foci appear in most teeth.
- On the tooth section in the cervical zone, a sharp waviness of the enamel-dentin boundary is detected. The structure of the enamel is not disrupted. The dentin layer is thinned, resembling interglobular dentin. In the cutting edge zone, interstitial denticle is detected. The tooth cavity is filled with denticles, with gaps containing pulp located between them.
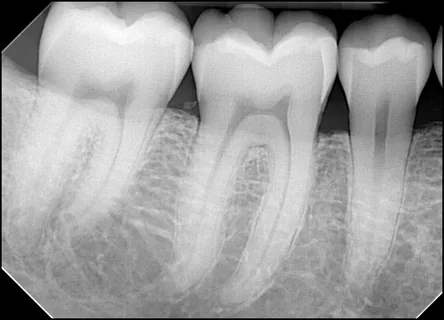
Figure 3. Dental X-ray.
Incomplete Odontogenesis
This is a hereditary disease that more commonly affects boys. The basis of the disease is insufficient mineralization of forming bones, including tooth tissues. The X-ray shows an excessively thin cortical layer, and the cancellous bone has a coarse trabecular structure.
The teeth are of normal size and shape. The color of the crowns varies from gray to yellowish-brown, with increased translucency. Histological examination confirms the normal structure of the enamel, but the enamel-dentin boundary resembles a straight line. The structure of the mantle dentin is correct, but as it approaches the pulp, the number of dentinal tubules decreases, and their lumen is sometimes narrowed or obliterated. The dentin is poorly mineralized.
Marble Bone Disease
The disease is characterized by complete or partial sclerosis of the spongy bone tissue throughout the skeleton. In the early stages of the disease, sclerosis of the bones is noted exclusively in the area of the metaphyses, as well as in the peripheral sections of the flat bones. The bones of the skull are unevenly densified. Usually, the paranasal sinuses are sclerosed. The development disorder of the jaw bones is associated with pathology in the development and timing of tooth eruption. Under the influence of the disease, teeth develop slowly, erupt late, and their structure is disrupted:
- roots are underdeveloped, canals and tooth cavity are obliterated;
- teeth are unable to resist the carious process.

Figure 4. Correction of crown shapes using a bridge prosthesis.
Hypophosphatasia
This is a hereditary disease, related to a group of metabolic disorders. The pathogenesis is based on a congenital pathology of alkaline phosphatase production. The diagnosis is made at the birth of the child, or within the first six months of life. Typical clinical manifestations include limb deformities, impaired calcification of the cranial vault bones, pathological fractures, cyanosis, dyspnea, vomiting, constipation, convulsive syndrome, and fragility of hair and nails.
From the perspective of the dental system:
- enamel hypoplasia;
- impaired development of tooth roots, accelerated resorption of them;
- early tooth loss.
The radiograph shows the insufficiency of the alveolar process, resorption of the roots of deciduous teeth, osteoporosis of the jaw bones.
Capdepont Dysplasia, Stanton-Capdepont Syndrome
This disease is characterized by normal shape and size of teeth, variable coloration, average eruption times. Enamel chips off almost immediately after eruption. The exposed dentin is heavily worn. The intensity of wear is determined by the severity of structural changes.
The teeth are almost unresponsive to various irritants. The roots have a normal shape and length. The tooth cavity and the channel lumen are greatly narrowed, often not visualized on an X-ray.

Figure 5. Early detection and treatment of hereditary tooth defects are important.
The basis of therapy for hereditary enamel disorders involves covering the teeth with crowns, with the choice of material depending on the tooth group. In cases of hereditary dentin pathology accompanied by tooth loss, removable dentures are indicated. For partial wear, teeth are covered with artificial crowns; in cases of complete wear, removable dentures are used. For the loss of several teeth, bridge dentures are recommended.
Detailed information about the shape and proportions of teeth at the Dental Aesthetics webinar.