
Tooth wear
Machine translation
Original article is written in RU language (link to read it) .
Erosion is called the process of loss of hard tooth tissues. Tooth erosion occurs both in temporary and permanent occlusions; both occlusal and approximal surfaces; both at a reduced and increased rate. Depending on the degree of manifestation of such a process, physiological and pathological erosions are primarily distinguished.
About types of pathological tooth erosion at the webinar Pathological Erosion. Classification. Diagnosis.

Physiological Tooth Erosion
Physiological tooth erosion has an adaptive nature and occurs as a result of regular contacts of antagonist teeth. The process begins from the moment the teeth enter into occlusal relations and, being slow-moving, continues throughout life. The adaptive aspect is that the teeth adapt to various movements of the lower jaw, ensuring the smoothness of its movements, reducing the load on the periodontium, and contributing to the integrity of the dental arch.
Due to the impact of contact points of antagonistic teeth on each other, areas are formed that increase the contact (or masticatory) surface of the teeth, facilitating the sliding of these teeth, reducing the amplitude of movements of the lower jaw, and decreasing the load on the temporomandibular joint.
The functions of the periodontium gradually decrease over the course of a person's life. This is due to a decrease in the trophic abilities of the neurovascular component of the periodontium, which leads to gradual atrophy of the alveolar bone, a decrease in the elasticity of fibers, and a change in the ratio between the intra-bone and extra-bone parts of the tooth. The tooth in the socket acts as a lever, and the larger its extra-bone part, the stronger the impact this tooth transmits to the periodontal tissues. Considering that there is a gradual loss of the bone part, the process should worsen over the years even in a person who does not have any pathological changes in the periodontium. But this does not normally happen. And it does not happen because the physiological wear of the hard tissues of the teeth reduces the height of the extra-bone part of the tooth. Thanks to this, the ratio of intra- and extra-bone parts of the tooth remains constant, and the load on the periodontium is adequate for the age.
In addition to occlusal surfaces, the approximal surfaces of teeth are also subject to natural wear. Interdental papillae also undergo atrophy over time and a reduction in their height. However, due to the transition of the point contact between the teeth into a planar one, the increase in the area of this platform and the approach of the lower edge of the platform to the gum, no gaps form between the teeth and the gum. This allows the body to perform adequate self-cleaning of the oral cavity and preserves the natural appearance of the teeth. Also, the increase in the contact surface increases stability in the dental row, and its shortening is compensated by the medial shifting of the teeth.
Thus, it is quite justified to conclude that physiological wearability is an interdependent property with the health of a person, an indispensable property of the human masticatory apparatus, contributing to the preservation of its functional and morphological integrity.

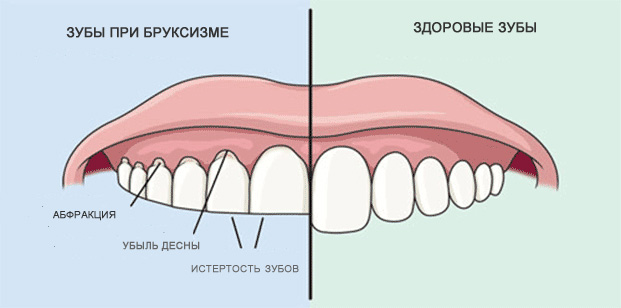
Pathological Tooth Wear
Pathological tooth wear, also known as increased wear, occurs when the wear of the teeth follows a pattern different from physiological wear. In pathological wear, the process ceases to be slow, involves the wear of other tooth surfaces, and, in addition to the enamel, the dentin and consequently the pulp of the tooth are also involved. Pathological wear is often accompanied by discomfort for the patient and the emergence of corresponding complaints, which almost never occurs in the natural process.
At the moment when wear transitions into a decompensated state, the height of the lower third of the face gradually decreases. This process is accompanied by dystrophic disorders in the temporomandibular joint, the appearance of pain in it and in the masticatory muscles, and a reduction in chewing function. Externally, this is manifested by the pronounced nasolabial and chin folds, a reduction in the lower third of the face, protrusion of the chin, and the person acquires what is called an aged facial expression.
Next, due to the upward displacement of the lower jaw, there is also a backward shift. In such cases, the breathing function suffers. The volume of the oropharynx decreases due to the distal displacement of the jaw, and consequently, its ability to pass the necessary volume of air. Reflexively, a person begins to slouch, dystrophic disorders occur in the spine, and consequently, primarily in the musculoskeletal and nervous systems of a person, as well as in the digestive, respiratory, cardiovascular, and other systems.
According to various estimates, due to the impairment of functions and condition of the masticatory apparatus and the changes described above, the reduction in a person's lifespan can occur by 15 years or more. Against such a background, smoking becomes a harmless pastime.

Causes of pathological tooth wear
The causes of pathological tooth wear are quite diverse. They can be grouped into the following categories.
Functional inadequacy of the hard tissues of the teeth, caused by a decrease in the qualitative and quantitative characteristics of enamel and dentin. In this case, the process can be:
- hereditary (e.g., Capdepont-Stenton Syndrome);
- congenital (disorders of amelo- and dentinogenesis);
- acquired (metabolic disorders of various etiologies, as well as disorders of the functions of the endocrine, vascular, nervous, and other systems)
The resistance to wear in teeth depends on the processes of calcification of the hard tissues of the tooth during the pre- and post-eruptive periods. The leading role in the mineralization processes is played by the neuro-humoral regulation of the body. Particularly important is the adequacy of the function of the parathyroid glands, responsible for the balance of calcium and potassium in the body.

Capdepont-Stenton Syndrome

Disorders of amelogenesis and dentinogenesis
Functional overload of teeth, which can occur in cases of:
- partial tooth loss;
- parafunctions (e.g., bruxism);
- hypertonus of masticatory muscles of various origins;
- chronic tooth trauma;
- malocclusions.
The pathology can be caused or exacerbated in cases where there are defects in the dental arches and parafunctions of the masticatory muscles. Missing teeth delegate their functions to the remaining teeth, and consequently, to their periodontium, causing its functional overload. This reduces the adaptive capabilities of the tooth's supporting apparatus, unable to compensate for the reduction in the height of the lower third of the face. In pathological wear, secondary cementum is deposited on the tooth root surface, remodeling in the alveolar bone tissue, and deformation of the periodontal gap occurs.
Along with this, the reduction in height can be accompanied by parafunctions of the masticatory muscles, manifesting as bruxism, hypertonus, etc. The reduction in height will inevitably lead to dystrophic changes in the temporomandibular joint. Since these processes are interconnected, a so-called "vicious circle" develops, where each element exacerbates another and the process as a whole. In such cases, establishing cause-and-effect relationships and creating plans for prevention and treatment becomes quite challenging.
Occupational hazards can arise in industries involving the release of acids, alkalis, and other substances, the intake of certain medications, etc. For example, acids reduce the quality characteristics of enamel and dentin, while fine dust is the most common abrasive, which, in combination with an adequate dental-jaw system, becomes aggressive, accelerating the processes of physiological wear.
Similarly, iatrogenic factors can also be the cause of increased wear, such as the high hardness of some ceramic masses used in prosthetics and poor polishing of restorations. Even in cases where the hardness of the materials does not exceed the hardness of the tooth tissues, their aggressive surface proves to be incomparable with the durability of the enamel, and even more so the dentin of the tooth.
Classification of Pathological Tooth Wear
Distinguishing a physiological process from a pathological one often is not difficult for a doctor, but the manifestations of pathological wear are quite diverse and require classification and specification in each specific case. Therefore, the classification of pathological tooth wear is as follows:
By stage (M.R. Bushan):
- physiological – within the enamel;
- transitional – within the enamel with partial involvement of the dentin;
- pathological – within the dentin.
Physiological wear always occurs within the dentin, however, in young age, enhanced enamel wear along with the etiological factor can be diagnosed by a doctor. Dentin wear is a characteristic sign of pathological wear. Involvement of the dentin can cause increased sensitivity and changes in the pulp, such as deposits of reparative dentin, narrowing of the root canal lumens up to the impassability of the canals, and pulp atrophy and formation of calcifications (denticles) in the tooth cavity.
By degree (M.R. Bushan):
- I – wear of 1/3 of the tooth crown length;
- II – wear of 2/3 of the tooth crown length;
- III – wear of the tooth crown more than 2/3.



In the absence of other factors contributing to periodontal diseases, pathological wear rarely accompanies changes in the supporting apparatus of the tooth. This is due to the reduction of the extra-bone part of the tooth and the reduction of the lever length, which decreases the load on the periodontium when the teeth are loaded.
By form (A.L. Grozovsky):
- horizontal;
- vertical;
- mixed.
In the horizontal form of wear, there is a loss of hard tissues of the teeth in the horizontal plane, forming horizontal wear facets. The process most often occurs on both the lower and upper jaws. The vertical type of wear is most characteristic and evident in the frontal group of teeth: on the palatal surface of the upper frontal teeth and the labial surface of the antagonists, which is determined by occlusal relationships. However, for example, in a progenic relationship of the jaws and dental arches, wear facets on the upper frontal teeth are observed from the labial side and from the lingual side of the antagonists.
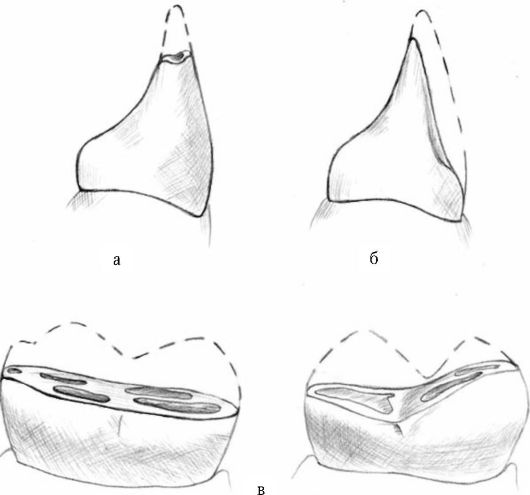
Forms of increased tooth wear: a — horizontal; b — vertical; c — mixed
By the degree of compensation (E.I. Gavrilov):
- compensated – without reduction in the height of the lower third of the face;
- decompensated – with a reduction in the height of the lower third of the face.
The dentomaxillary system has relatively high compensatory capabilities. Following the loss of hard tooth tissues, there is a restructuring of the alveolar processes of the jaws and displacement of teeth towards the defect area or the area lacking occlusal relationships. This is known as tooth-alveolar elongation, or the Popov-Godon phenomenon. Depending on the degree of such restructuring, pathological tooth wear is differentiated into compensated, when tooth displacement prevents a reduction in the height of the lower third of the face, and decompensated, when compensatory restructuring is either unable to fully eliminate the defect or is completely absent.
By extent (V.Yu. Kurlyandskiy):
- localized – increased wear of individual teeth or groups of teeth;
- generalized.
Localized wear is more often observed in the frontal section of the dental rows, for example, in cases of deep bite. This type of wear is also locally compensated by the body thanks to local hypertrophy of the alveolar process. In such cases, the support points of the lower third of the face, which fall on the molar teeth, remain intact, without disruption of occlusal relationships and the position of the elements of the temporomandibular joint.

In the generalized form of the process, the crowns of all teeth are involved with disruption of the bite height. In such cases, the degree of compensation depends on individual characteristics of the organism.

Learn more about effective methods of treating patients with pathological erasability in the online course Pathological Erasability: Treatment.