
Clasp denture fixation systems
Machine translation
Original article is written in RU language (link to read it) .
Most students and patients, upon hearing the term "clasp denture," first imagine a removable metal "part" with plastic teeth and an artificial gum, which is held quite firmly on the teeth using a clasp system of the clasp denture.
Learn more about various types of removable denture fixations in the online course Removable Prosthodontics using Exocad: Bar, Screw, and Telescopic Designs.
For each point in this presentation, an alternative can be found: the framework can be non-metallic, the teeth not acrylic, and the gums not plastic, but in this case, we are interested in the aspect related to clasps, as they have a number of alternatives that often turn out to be superior both functionally and aesthetically compared to these very clasps. Thus, among the fixation systems of the clasp denture, the following are distinguished:
- clasp system;
- lock attachments (attachments);
- telescopic system;
- bar system, or Rumpel-Schroeder-Dolder system;
- magnetic system.

And systems other than the clasp system provide quite significant and important alternatives, surpassing the first in quality in the clinical situations shown. Yes, clasps are the most popular fixation system, which is due to a combination of their relatively low cost, comparative ease of manufacture, and very acceptable functional results. And since they occupy such an important position in removable partial denture prosthetics, let's start with them.
Clasp System — Clasp Denture
The clasp system is the most common system for fixing and stabilizing a clasp denture. In a clasp denture, the clasp is supportive and retentive, which means that the tooth not only serves to hold the denture in place but also absorbs part of the chewing load that falls on the denture.
The multitude of types of clasps has led to the need for their systematization, so in the first half of the last century, the Ney clasp system was developed in the USA, which combined 5 types of clasps.
Ney Clasp System
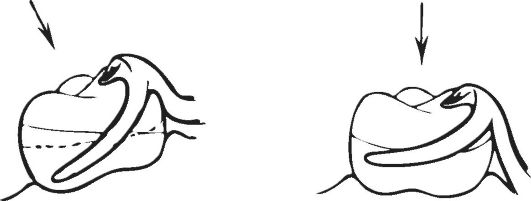
Type I clasp – Acker clasp
The Acker clasp is most convenient for examining the structure and function performed by clasps in general.
In the clasp, three parts are distinguished:
- the arm, which is adjacent to the tooth and performs a supportive and retentive function;
- the occlusal rest, which is located on the occlusal surface of the tooth and transfers part of the chewing pressure to the supporting tooth;
- the body — the area where the arm and the occlusal rest of the clasp converge;
- the extension, connecting the clasp to the framework of the clasp denture.
The anatomical shape of teeth includes an equator, which can also be recreated with prosthetics if necessary. The equator divides the tooth into two parts: the subgingival, located between the edge of the gum and the tooth's equator, which is also called the retention or holding area, and the supporting area, located above the equator up to the occlusal surface of the tooth. As we remember, the clasp arm in a plate denture was located below the tooth's equator, so the clasp only performed a retaining function (being in the retention zone), but the clasp in a partial denture is more complex.
The clasp arm "embraces" the tooth, being simultaneously in the retention (retaining part of the arm) and supporting zones (stabilizing part of the arm), thereby performing a supporting-retaining function and is accordingly named. The retaining part of the arm is not capable of transmitting chewing pressure to the supporting tooth, so it only participates in the retention of the denture and resists the displacement of the denture in the occlusal direction. The stabilizing part of the arm "lies" on the tooth surface, preventing the denture from sinking towards the gum.
Thanks to the elastic properties, the clasp arm can overcome an obstacle such as the equator and reach the retaining area. However, sometimes this elasticity is not enough, so a second type of clasp comes to the rescue.
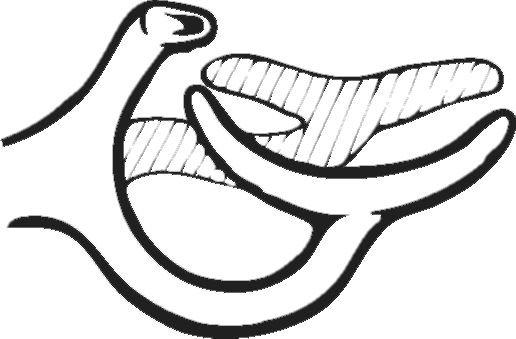
Type II clasp – Roach clasp
Unlike the Ackers clasp, the arm in the Roach clasp, deviating from the body, first heads towards the gum, where after a semicircular bend it moves towards the retention area and ends there with a T-shaped branching. This shape makes the arm longer and, as a result, less rigid than the arm in the Ackers clasp. This shape allows the retaining part of the arm to be positioned in a tooth with a small retention area, or in teeth, when the close position of the equator to the occlusal surface leaves no room for the stabilizing part of the Ackers clasp. Also, the Roach clasp is more aesthetic compared to the previous one, as most of the arm is moved off the tooth surface.
However, the Roach clasp is not without its drawbacks. These include weak stabilizing action, due to the weak coverage of the supporting part of the tooth and less rigid arms, which is partially compensated by a larger occlusal overlay area. Pronounced bone protrusions can interfere with the clasp arm located above the gum, and its lesser rigidity may lead to bending if the denture is handled carelessly.
Type III clasp – combined Ackers and Roach clasp
With a pronounced tilt of the tooth, one can observe that one surface (facing the direction of the tilt) is more suitable for the Roach clasp, as the tilt makes the equator even more pronounced, while the other surface favors the placement of the Ackers clasp. The strongly pronounced equator on the side of the Roach clasp gives it even more retaining properties. On the side of the Ackers clasp, the equator approaches the gum, which increases the area of the support zone and the degree of the corresponding action of the clasp. Thus, the lack of either support or retention function is compensated, making such a clasp design most favorable for pronounced tilts of the molar teeth.
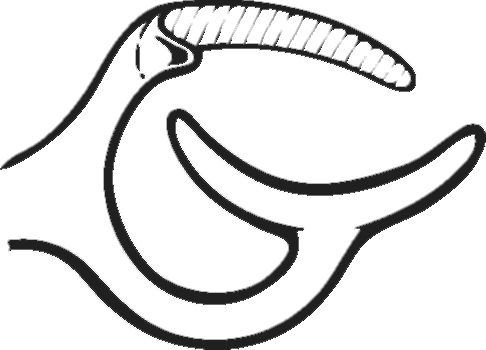
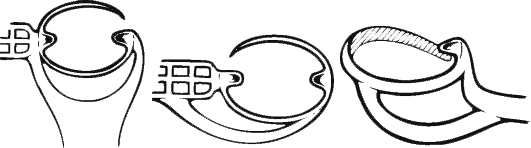
Type IV Clasp – Distal Action Clasp
When molars are lost, premolars used as abutment teeth are subjected to immense stress, thus increasing the likelihood of their dislocation. However, the design of the distal action clasp allows for the redistribution of applied forces, primarily into the mesial area of the occlusal surface of the crown. In this case, the tooth does not dislocate from the socket but instead moves into the socket along a path close to the longitudinal axis of the tooth.
The design that allows for such an application of forces consists of a single arm starting from the body and encompassing the oral, mesial, and buccal surfaces of the crown with the occlusal overlay positioned on the mesial side of the occlusal surface of the tooth. On the oral side, the arm does not cross the tooth's equator, thus serving as a stabilizing part of the arm at this location. The retention part is the portion of the arm that is located under the marginal line on the buccal side and prevents the prosthesis from shifting in the occlusal direction.
From this structure, it follows that the stabilizing part of the arm significantly prevails in length over the retention part, which implies that the stabilization of the prosthesis will be weakened. Therefore, such a clasp design has found its application on premolars with a subsequent terminal defect on the lower jaw, where the retention of the prosthesis is not as crucial as on the upper jaw.
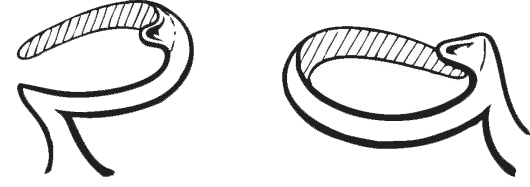
Type V clasp – ring clasp
The ring clasp is designed for standalone molars, may have one or two occlusal pads, and has design features for molars of the upper or lower jaw.
Any standalone teeth used as supports have an increased and quite real risk of being dislocated, which is why it is important to properly distribute the load on them to minimize the predominance of the load on one side, and, as a result, the threat of dislocation. This can be achieved by distributing the areas of force application around the perimeter of the tooth through one encompassing arm and two occlusal pads — mesial and distal.
This clasp begins with an arm on the side of the defect, and the further course of the arm varies depending on whether the molar belongs to the upper or lower jaw. Upper jaw molars have a more pronounced tilt towards the buccal side, i.e., they diverge, while lower jaw molars tend to converge, i.e., have a lingual tilt. As a result, there is a relationship between the tilt and the placement of the retentive and stabilizing parts of the arm, similar to the combined Ackers and Roach clasp discussed above. On upper jaw molars, the stabilizing part of the arm is located on the palatal surface, encompasses the approximal surface, where it may have a "projection" in the form of an occlusal overlay, and transitions into the retentive part of the arm on the buccal side. The clasp on lower jaw molars has the opposite design – it starts with the stabilizing part on the buccal surface and ends with the retentive part on the lingual side.
The Ney system does not cover all types of clasps. There are many modifications of clasps both from the Ney system and completely different designs, however, by describing the Ney system specifically, one gets an idea of the essence of clasps in general.

Locking Attachments — Removable Partial Denture on Attachments
In addition to clasps, the ability to retain a tooth and transmit chewing pressure to it is possessed by locking connections, or attachments. Despite the difficulties that may arise when using attachments in the construction of removable partial dentures, they are an excellent replacement, and quite often the element of choice, considering their positive aspects.
So, attachments are small lock fasteners, the connection of which is provided by a matrix on one side and a corresponding die on the other. Here lies the first difference of attachments - they can be intradental, when the lock fasteners connect inside the volume of the tooth, or extradental, when the elements are connected outside the tooth.
Intradental connections are more physiological in relation to the periodontium of the tooth, as the dislocating force is minimal, however, the manufacture of such a structure requires a greater volume of preparation of the hard tissues of the tooth, and sometimes even depulpation of the tooth. If depulpation is necessary in relation to the tooth, or more precisely to its pulp, an extradental lock connection will be more physiological, however, the points of force application are located at a greater distance from the longitudinal axis of the tooth, which results in greater dislocating forces, compared to the first option. An extradental connection will favorably affect the integrity of the tooth due to the preservation of counterforts, which protect the tooth from fracture and internal redistribution of pressure, however, the dislocating moment will gradually adversely affect the periodontium of the supporting tooth.
Another difference in clasp attachments is their mobility, varying degrees of which are used depending on the topography of defects and the condition of the periodontium of the supporting teeth. For example, in defects of Class I and II according to Kennedy (bilateral and unilateral terminal respectively) or when there are concerns about the progression of destructive changes in the periodontium, the use of mobile clasp connections: rotational or hinge, is justified. For included defects (Class III and IV according to Kennedy) and a strong periodontium of the supporting teeth, fixed clasp connections are used.
Among the positive qualities of attachments, their inconspicuousness is important, and as a result, the aesthetics of prostheses in the oral cavity. Clasp attachments allow partial dentures to be considered semi-physiological because part of the chewing pressure is transmitted to the periodontium of the supporting teeth, and they do this successfully. In addition, clasp attachment as an engineering structure is more complex, as it requires tooth preparation, and sometimes significant. They are also finicky about the clinical height of crowns, as well as their buccal-lingual dimensions, which is why the use of attachments may be limited in cases of tooth wear and when the crown height is less than 5-6 mm and in the anterior group of teeth, where the buccal-lingual dimensions are smaller than those of the molar teeth.
As mentioned above, the use of clasp attachments requires the preparation of abutment teeth, and the downside is not only the fact of damaging the hard tissues of the tooth, but also their further covering with special crowns, which is an additional cost for the patient, considering that the crowns must also be aesthetic, in order not to lose one of the advantages of the clasp denture design using clasp attachments – their appearance.

Telescopic System for Fixing Clasp Dentures — Telescopic Clasp Denture
The use of telescopic crowns, and accordingly telescopic fixation of clasp dentures, is a kind of clasp attachment, however, it significantly exceeds the latter in functional qualities.
The essence of the telescopic crown is that it is a double crown, where the primary crown is non-removable and directly covers the tooth, while the secondary crown is rigidly connected to the framework of the removable partial denture and performs both a supportive-retentive function and compensates for aesthetic and functional deficiencies, if any were present.
The basis of high functional qualities lies in the high degree of correspondence between the primary and secondary crowns to each other, which is achieved through high-precision precision casting technologies. After preparing the abutment teeth, taking impressions, and sending them to the laboratory, the dental technician models the primary crowns on the abutment teeth, achieving the maximum possible parallelism of the walls, as this aspect is easier to recreate in the controlled conditions of the laboratory and with models in hand, than in the limited conditions of the oral cavity. In addition to excellent fit to the tooth and recreating the parallelism of the walls, the primary crowns must be perfectly polished for further high-precision modeling of the inner surface of the secondary crowns. The inner surface of the secondary crown, which adjoins the primary, is modeled using modeling plastic to eliminate distortions that could arise when using wax, which is used for modeling the remaining part of the crown or its framework for subsequent aesthetic facing with plastic or ceramics.
The next stage can proceed in different directions. One of them is the separate modeling and casting of the secondary crown followed by its rigid connection to the framework of the removable partial denture. With such a connection, there is a possibility of the crown shifting, which will undoubtedly reduce all the positive qualities achieved by precise modeling and precision casting. To avoid this, there is a second option where the crown and the framework are connected while still being modeled, and then cast together.
In principle, the disadvantages of telescopes are similar to those of attachments: the need for tooth preparation with possible depulpation and increased cost of the prosthesis. However, this type of retention elements has undeniable advantages over attachments, consisting in the maximum support-retention properties among all retention elements, as well as high aesthetic qualities.

Beam Fixation System
Following lock fasteners and telescopic fixation, the beam fixation system, or the Rumpel-Schroeder-Dolder system, continues the ideology of the matrix-patrix construction. This time, the patrix is a beam that extends over the alveolar ridge from the crown part of one tooth to another, and the corresponding matrix is located on the inner surface of the removable denture.
An important advantage of the "beam" is that it acts as a permanent splint, which by connecting the remaining teeth located in different segments of the dental row, enhances their stability and allows them to withstand greater pressure, as well as creates conditions for reliable fixation of the denture on this very "beam".
The beam can be placed almost anywhere, of course, except in a diagonal position. In such a case, it can be frontal, sagittal, frontosagittal, or arch-shaped, combining all three sections of the dental row. In shape, it can also vary and be elliptical, rectangular, or, for example, pear-shaped in cross-section. The most functionally acceptable and durable will be the arch-shaped, however, the clinical picture does not always allow for the positioning of the supporting teeth to connect them with the creation of a large "beam", but such a beam requires a strong periodontium of these teeth, as well as a larger number of them. At the same time, closely located teeth illogically combined with a "beam", whereas telescopic fixation will become a better alternative.
Undoubtedly, such a system cannot always be applied, it is quite bulky, complex to manufacture and adversely affects the cost of the prosthesis, but if there are indications for it, it will surely be the best option, as it will treat the periodontium of the remaining teeth most gently, while providing reliable fixation and high functional qualities.

Magnetic fixation system
The technical part is not difficult to understand, how the magnetic fixation system works. And this technical part is quite simple – poles with opposite charges attract, poles with the same charges repel.
In any removable prosthesis, it is necessary for the prosthesis to be attracted to the tissues of the prosthetic bed, and accordingly, to be repelled from the opposite side, which can be a prosthesis from the second jaw.
In order for the prosthesis to be attracted to the tissues of the prosthetic bed, one pole with a certain charge must be placed under these tissues, which is done surgically by implanting magnetic implants, and the pole with the opposite charge must find its place in the prosthesis itself.
However, poles with the same charge can also be used as a fixation system. In this case, magnets with the same charge are placed in both removable prostheses for both jaws. As a result, their repulsion from each other will contribute to the compression and thus better retention of both prostheses on the tissues of the prosthetic bed.
About the specifics of planning beam structures in the webinar Laboratory stages of manufacturing removable prostheses.