Mesial occlusion. Etiology, diagnosis, correction.
Machine translation
Original article is written in RU language (link to read it) .
Mesial occlusion represents a pathology of occlusion in the sagittal plane, characterized by the following features:
- when the dental rows are closed, the buccal-mesial cusp of the first upper molar is located behind the intercuspal fissure of the opposing tooth;
- the upper canine is positioned behind the interdental space between the lower canine and premolar.
About the causes and principles of treatment of mesial occlusion in the webinar Open and Mesial Occlusion. Etiology. Treatment Approaches.
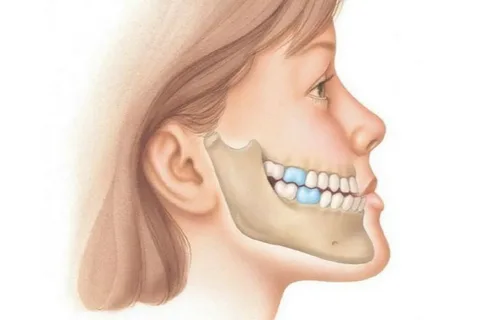
Figure 1. Mesial occlusion.
Alternatively, "mesial occlusion" is also called prognathic or simply prognathism, it belongs to Class III according to the Angle classification, it is also mesioocclusion.
Causes of Mesial Occlusion
Most often, prognathic occlusion is a pathology determined by a hereditary factor, the patient is diagnosed with genetically determined upper micrognathia or lower macrognathia.
Among congenital factors, the following can be highlighted:
- birth trauma;
- developmental defects accompanied by cleft palate.
Acquired factors include:
- adentia,
- on the lower jaw – supernumerary teeth;
- on the upper jaw – aneruption of teeth;
- macroglossia;
- improper sleeping posture;
- presence of harmful habits (sucking the upper lip, foreign objects, habit of thrusting the lower jaw forward);
- premature loss of teeth on the upper jaw due to complicated caries and other factors;
- impaired wear of cusps at the stage of temporary occlusion;
- inflammatory diseases of the jaws.
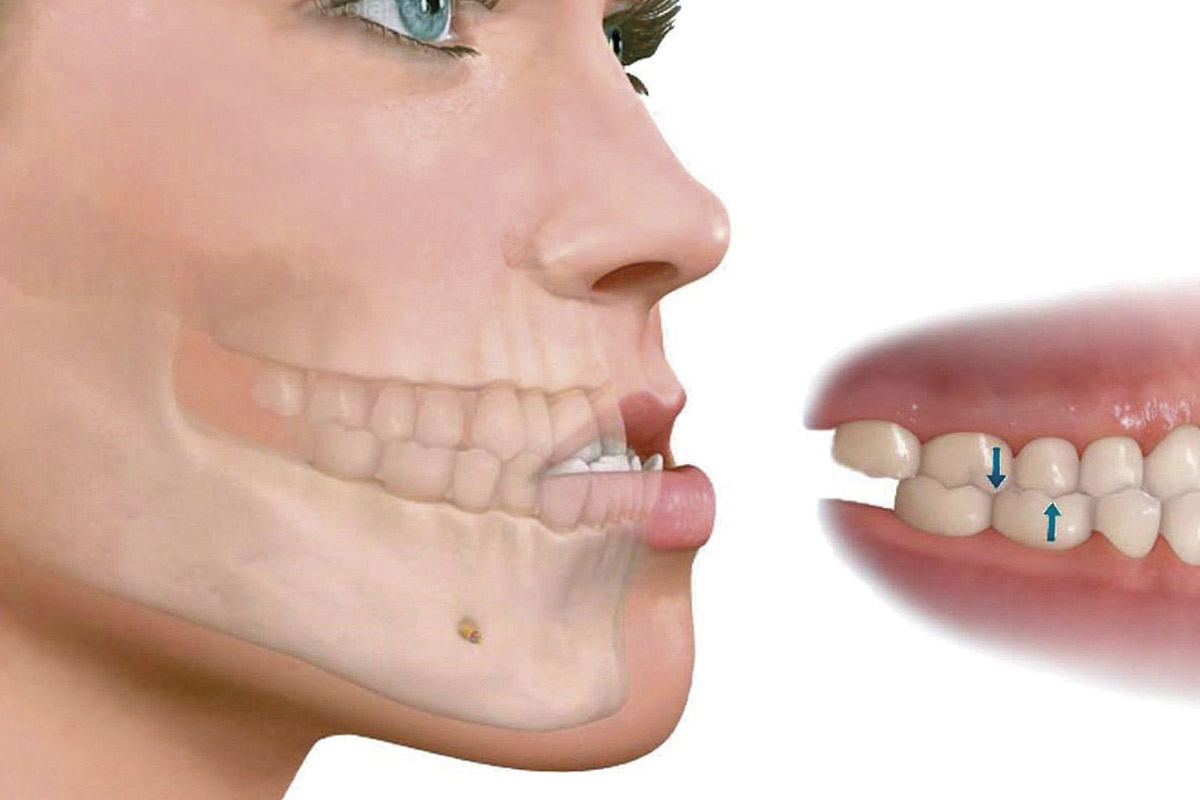
Figure 2. Feature of a mesial occlusion.
External features of mesial occlusion
In profile, the patient's face with a prognathic occlusion appears concave, characterized by a protruding chin, a recessed upper lip, an enlarged lower facial section (against the background of a reverse deep incisal overlap, the lower third of the face may be reduced), deepening of the nasolabial fold, and thickening of the lower lip.
The following morphological forms of progenic occlusion are distinguished:
- dentoalveolar,
- gnathic,
- combined.
This occlusal disorder may also be accompanied by a displacement of the lower jaw, or the mesial occlusion may occur without displacement of the latter.
At the level of the jaws in the dentomaxillary system, characteristic morphological disorders appear:
- the upper jaw occupies a posterior position, this is called retrognathia;
- the upper jaw is reduced in size (micrognathia);
- the lower jaw occupies an anterior position (prognathia);
- the lower jaw is somewhat enlarged in size (macroganthia).
At the level of dental arches in mesial occlusion, characteristic changes include:
- the upper dental arch is shortened in the frontal section;
- the lower dental arch is lengthened in the frontal section.

Figure 3. External features of mesial occlusion.
At the level of teeth, for prognathic occlusion, it is characteristic:
- lower molar teeth shift mesially.
In mesial occlusion at the level of the dental-jaw system, some functions suffer:
- biting is difficult;
- the process of chewing is disrupted;
- swallowing is impaired;
- articulation of the tongue is difficult;
- problems with the pronunciation of many sounds arise.
Principles of Diagnosis of Prognathic Occlusion
The basis of the diagnosis of mesial occlusion and its varieties involves the use of techniques:
- clinical examination;
- conducting functional clinical tests;
- technique of studying diagnostic models;
- studying photographs of the face;
- evaluation of orthopantomograms;
- analysis of lateral cephalometric radiographs.
The technique of studying diagnostic models in patients with mesial occlusion involves:
- analysis of the correspondence of the length of the dental arch to the sum of the sizes of all its teeth (Nance, Lundstrom techniques);
- determining the length of the anterior segment of the dental arch (according to Corkhaus);
- measuring the width of the dental arches (according to Pont);
- analysis of apical bases (Snagina technique);
- studying the ratio of the sizes of fragments of dental rows (according to Gerlach).
The performance and subsequent study of lateral cephalometric radiographs allows for the assessment of morphological changes in the structure of the facial skeleton bones, determine the type of growth, and establish the growth period of the bones.
To differentiate the dentoalveolar form of prognathic occlusion from the gnathic form, a diagnostic test is used during the clinical examination: the patient is asked to retract the lower jaw back until the incisors are completely occluded. If at this point the first molars are positioned in a typical neutral occlusion, then the patient is confirmed to have a dentoalveolar form of prognathic occlusion with forward displacement of the lower jaw.
Principles of treatment of mesial occlusion at different periods of occlusion formation
Treatment of prognathism begins early, already at the age of three, at this stage it is important to eliminate acquired factors that caused this anomaly.
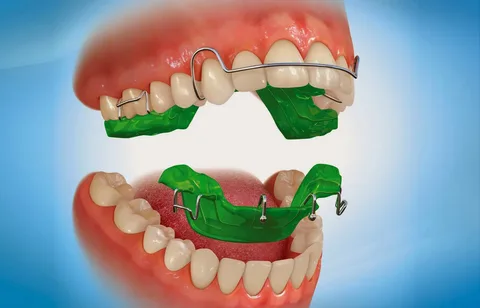
Figure 4. Hardware treatment method.
Temporary occlusion stage
At this stage, the main goal is to create favorable conditions for the growth and increase in size of the upper jaw while restraining further development of the lower jaw.
The primary method of treatment is hardware-based, with myotherapy as an additional method. In rare clinical situations, a comprehensive method is preferred.
The choice of treatment tactics is also determined by the size of the reverse incisal overlap and the dimensions of the sagittal gap.
- If the incisal overlap does not exceed half the height of the crown of the temporary incisor, grinding of the incisors and canines on both jaws is performed. This procedure can be done in one go or over several visits, depending on the psycho-emotional state of the young patient and the sensitivity of their teeth. After grinding, remineralization therapy is mandatory. To restrain the growth of the lower jaw, the most effective device at the stage of temporary occlusion is considered to be a cap with a chin strap and sagittal rubber traction. If a mesial bite is combined with protrusion of the lower jaw incisors, as well as anomalies in functions, standard and individual vestibular plates are additionally used.
- If the incisal overlap exceeds half the height of the crown of the temporary incisor, in addition to grinding the canines and incisors, disoccluding devices are used. For children who cannot adapt to orthodontic appliances, teeth that block the development of the upper jaw are removed, and then the child needs to use extraoral devices that restrain the growth of the lower jaw.
Mixed Dentition Stage
At this stage, the main goal is to optimize the development of the upper jaw and slow down the growth of the lower jaw in the sagittal plane.
The primary treatment method is appliance-based, with myotherapy used as an additional method. In rare clinical situations, a comprehensive approach is preferred.
Permanent Dentition Stage
The main goal of the comprehensive method at this stage is to reduce the length of the lower dental arch to optimize the relationship between the dental arches. The main treatment methods are surgical, comprehensive, and appliance-based. The latter is indicated exclusively for minimal sagittal discrepancies (sagittal gap not exceeding 5 mm), associated with the posterior position of the upper jaw and its slow development.
Contraindications for the comprehensive method
- Macrogenia, which cannot be corrected by reducing the size of the lower dental arch. Surgical treatment is necessary.
- Macroglossia. The volume of the oral cavity decreases due to the extraction of teeth in the lower jaw, the pressure of the tongue on the lower jaw increases, leading to a recurrence of disorders.
- Tremas, diastemas in the frontal section of the lower jaw – these are signs of macroglossia or macrogenia.
- A significant oral inclination of the lower anterior teeth leads to their inability to withstand axial load, making them prone to dislocations during biting.
Most often, a multibonding system is used to correct prognathism as part of a comprehensive method during the period of permanent occlusion. In cases of significant sagittal discrepancy against the background of maxillary micrognathia and mandibular macrognathia, surgical treatment is indicated.

Figure 5. Treatment using the multibonding system.
The multibonding system helps optimize the position of individual teeth and normalize the shape of the dental arches.
To prevent recurrence after the end of orthodontic treatment during the period of permanent occlusion, it is recommended to remove the germs of the third molars on the lower jaw. This serves as a prevention of the growth of the lower jaw, as well as the appearance of tooth crowding in the frontal section.
Learn more about the treatment tactics of mesial occlusion at the stage of mixed occlusion in the webinar Mesial occlusion in mixed occlusion: diagnosis and treatment.