Etiology and Clinical Presentation of Open Bite
Machine translation
Original article is written in RU language (link to read it) .
Open bite represents one of the types of malocclusion, a pathology of occlusion in the vertical plane, where the patient has a vertical gap when closing the jaws between the teeth.
Clinical cases of open bite are discussed in the webinar Open Bite: Skeletal and Dentoalveolar Forms.
This gap is predominantly located in the frontal section, it can be symmetrical and asymmetrical, in the case of localization in the area of the chewing teeth, unilateral and bilateral vertical gaps are distinguished.
The absence of interocclusal contact can be diagnosed exclusively in the area of the front teeth, but sometimes the pathology is more extensive, in which case the absence of contact can even be observed in the area of premolars and some molars. In the patient, the closure of the dental rows occurs only in the area of the last teeth.

Figure 1. Appearance of a patient with an open bite.
Etiology of the Disease
Among the etiological factors of open bite, the following are of primary importance:
- Hereditary factors.
- Congenital pathological conditions (birth trauma, fetal position anomalies, maternal diseases).
- Acquired anomaly.
The latter, in turn, is conditioned by a number of local factors:
- the harmful habit of sucking various objects, including one's own fingers, lips, tongue;
- head tilted back during sleep;
- early removal of temporary teeth, habitual position of the tongue in the area of the dental arch defect.
Nasal breathing problems are of great importance, where the patient is forced to spend a long time with an open mouth, in which case the tongue almost always occupies an incorrect position, being placed between the teeth. With chronic lesions of the pharyngeal tonsils, the tongue shifts forward, this position becomes habitual for the patient and an open bite develops.

Figure 2. Placing the tongue between the teeth.
With a short lingual frenulum, the movements of the tongue are hindered, which contributes to the incorrect positioning of the tongue. Speech formation pathology (caused by abnormal tongue articulation) delays the timely eruption of teeth, creating favorable conditions for the formation of an open bite in the frontal section.
The size and configuration of the tongue at the embryonic stage of oral cavity development can lay the foundation for future bite anomaly - open occlusion, predominantly in the area of the molars.
The development of an open bite is possible at any age of the patient. It can be diagnosed against the background of a neutral bite, as well as in combination with other occlusion pathologies - distal or mesial bites.
Clinical Course Features
The severity of clinical manifestations of an open bite depends on the size of the gap in the vertical plane:
- 1st degree — the size of the gap does not exceed 5 mm,
- 2nd degree — the size of the gap is about 5-9 mm,
- 3rd degree — the size of the gap exceeds 9 mm.
In cases of open bite, the following morphological changes are noted at the level of the jaws:
- the body of the upper jaw rotates along the horizontal axis upwards and forwards;
- the lower jaw rotates with its body downwards and backwards.

Figure 3. Clinic of open bite.
The following morphological disturbances are highlighted at the level of the dental arches:
- extrusion of teeth is observed in the area of the molar teeth of both jaws;
- intrusion is noted in the area of the frontal teeth of both jaws;
- supraocclusion – in the area of the lower molar teeth;
- infraocclusion – in the area of the upper molar teeth.
With a large vertical gap exceeding 8 mm, the patient exhibits a facial configuration disorder, with the lower section prevailing over the other two, a protruding tip of the tongue visible, and the upper lip shortened. The angle of the lower jaw is more than 135°. With lips closed, the facial expression is very tense.
If an open bite is combined with other types of pathological occlusion, additional facial features characteristic of these bite anomalies are noted.
Characteristics of the clinic typical for open bite:
- narrow dental arches,
- crowded, tight position of the frontal teeth,
- frequently accompanied by enamel hypoplasia.
Functional disorders associated with open occlusion:
- difficulty in biting off food,
- problems with chewing food, swallowing, speech formation are noted,
- breathing is impaired,
- xerostomia often occurs.
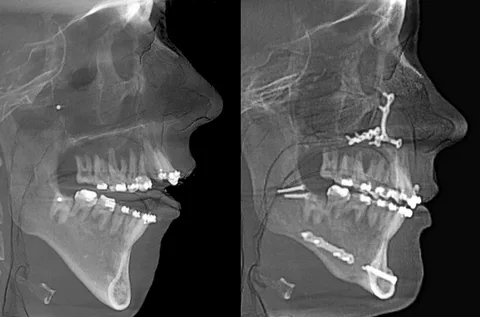
Figure 4. Diagnosis of open bite.
Diagnosis
The diagnosis is made based on a combination of the following diagnostic measures:
- thorough clinical examination,
- orthopantomography of the jaws,
- facial photometry,
- lateral cephalometric radiography,
- determination of gnathic and dental-alveolar forms.
Features of treating open bite
The set of measures taken to correct an open bite is determined by the type of this pathology, the degree of clinical manifestations in a specific patient, the period of formation, and the characteristics of jaw growth.
At the stage of temporary bite, the main task is to rid the patient of existing harmful habits, optimize the usual position of the tongue, establish nasal breathing, ensure lip closure, normalize swallowing of food and speech formation. If necessary, during this period, surgical plastic surgery of the short lingual frenulum is performed. To rid the patient of harmful habits, individual or standard plates are made. A vestibular plate with a tongue stop helps eliminate the habit of tongue sucking, optimizes swallowing. At this stage, the grinding of molar teeth is also carried out.
At the stage of mixed dentition, all the above-mentioned treatment measures can be used, which are indicated during the temporary dentition. To rid the patient of the harmful habit of sucking or pushing the tongue into the dental row defect, a plate is made for the upper jaw, equipped with a wire stop, which helps to normalize the position of the tongue.
Throughout this period, devices are used, taking into account the main type of pathology in the patient (mesial or distal occlusion). The tongue is distanced from the teeth thanks to wire loops located at the level of the vertical inter-incisor gap. The devices used at this stage provide gradual expansion of the dental rows, predominantly the upper, which is a crucial stage in correcting an open bite. Dental alveolar traction is achieved by attaching rubber traction.
Treatment at the stage of permanent occlusion involves a comprehensive approach, which includes the use of surgical and device methods. If necessary, tooth extraction is indicated in cases of their crowded and tight position, compact osteotomy is performed, and various devices are made, both removable and non-removable. Among the latter includes the multibonding system in conjunction with reversion arches.
In some clinical situations at the stage of permanent occlusion, the use of a prosthetic method is indicated, provided there is a sufficient size of the upper lip, moderately sized mandibular angles, and a minor elongation of the lower part of the face.
The duration of treatment for open occlusion is determined by the period of occlusion formation, its type, the severity of functional disorders, the possibilities for their correction, and the extent of morphological changes.

Figure 5. Bite correction using a multi-bonding system.
In cases where the patient has a dental alveolar form of this bite, the prognosis for treatment will be more favorable compared to the gnathic form. The final result of the treatment is determined by the age of the patient at the time treatment began. If functional disturbances were not completely corrected during comprehensive and appliance treatment, there is a high likelihood of relapse. The prognosis for eliminating the gnathic form depends on the degree of jaw deformation.
Mistakes in treating an open bite
In the process of treating an open occlusion at various stages of bite formation, the following possible mistakes are encountered:
- Deterioration of facial harmony, where during a smile not only the teeth but also the alveolar processes are exposed, observed when the lower third of the face is elongated, and intrusion in the area of the molars was not performed, with the correction of the open bite occurring solely through the elongation of the front teeth.
- Using excessive force to move teeth can provoke painful sensations in the teeth, lead to their loosening, gum recession, and possible changes in tooth color due to bleeding in the pulp.
- A mistake is to elongate teeth when they are closely positioned. It is necessary to ensure the expansion of the dental arch and correct the tight positioning of the teeth by removing some of them.
Distalization and intrusion of molars using microimplants in the webinar Open bite, gummy smile: treatment using microimplants. Aligners + skeletal support.