
Interdisciplinary Approach to the Diagnosis and Treatment of Sublingual Syndrome: Initial Experience
Machine translation
Original article is written in RU language (link to read it) .
In order to improve the methods of diagnosis, differential diagnosis, and surgical treatment of the stylohyoid syndrome, an analysis of the literature data was conducted, a retrospective analysis of radiological data was performed, and an examination algorithm and a minimally invasive surgical treatment method for this disease were implemented into clinical practice.
Relevance
The difficulties in diagnosing the stylohyoid syndrome are due to the absence of characteristic complaints and pathognomonic clinical signs; therefore, as a rule, the diagnosis is made by excluding neurological, otorhinolaryngological, and dental pathologies. The syndrome causes suffering to patients, reduces the quality of life, and impairs work capacity. The need to improve medical care for patients with stylohyoid syndrome determines the social significance and relevance of the problem of diagnosing and treating this disease. The presence of clinical and radiological data in favor of establishing this diagnosis is an indication for surgical treatment of the syndrome — resection of the styloid process and the calcified stylohyoid ligament. Various surgical access options have been proposed for performing the resection of the styloid process: an incision in the submandibular area; an incision encircling the angle of the mandible; an incision in the hairy part of the occipital region; an intraoral incision in the area of the pterygomaxillary fold and the anterior palatine arch; an incision in the area of the tonsillar fossa with simultaneous tonsillectomy. To reduce trauma and achieve the best cosmetic result during such operations, endoscopic equipment is used. Minimizing surgical trauma and the duration of the operation is also facilitated by the use of surgical navigation equipment.
Objective
Improvement of diagnostic methods and surgical treatment of the hypoglossal syndrome.
Materials and Methods
From 2017 to 2019, 100 patients aged 48.4±19.5 years (50 men and 50 women) underwent examination and treatment at the clinic of maxillofacial surgery of the First Saint Petersburg State Medical University named after acad. I.P. Pavlov, due to complaints characteristic of hypoglossal syndrome. The diagnostic examination algorithm included: a survey, objective examination by a maxillofacial surgeon, multi-slice computed tomography of the maxillofacial area and cervical spine, consultations with a neurologist and an otorhinolaryngologist.
The inclusion criteria for the study were:
complaints of constant dull pain in the deep area of the face and the upper part of the anterior and lateral regions of the neck;
patients of both genders aged 18 to 80 years.
Native CT study was performed using a 16-slice computed tomography scanner Optima 540 CT (General Electric) according to the standard protocol with a slice thickness and increment of 5 mm, followed by reconstruction at 1.25 mm in mediastinal and bone windows to exclude inflammatory, traumatic, and destructive changes in the bones of the maxillofacial region and cervical spine, soft tissue formations of the maxillofacial region and neck. The evaluation of the obtained radiological data was carried out by constructing multiplanar and volumetric reconstructions. The length of the styloid processes was measured on the right (RSP) and left (LSP) on the multiplanar reconstructions based on the CT data (fig. 1, 2).
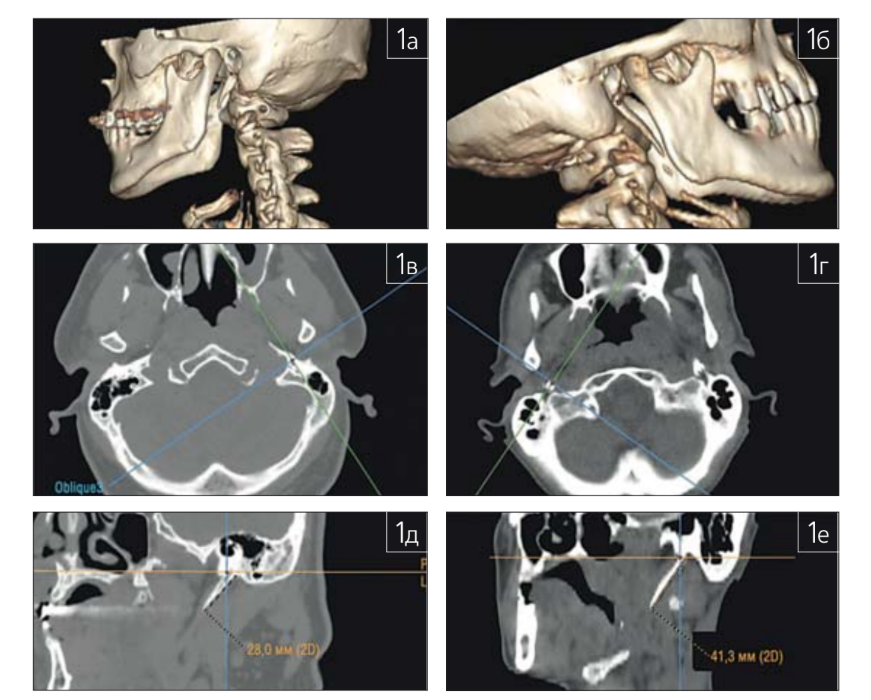
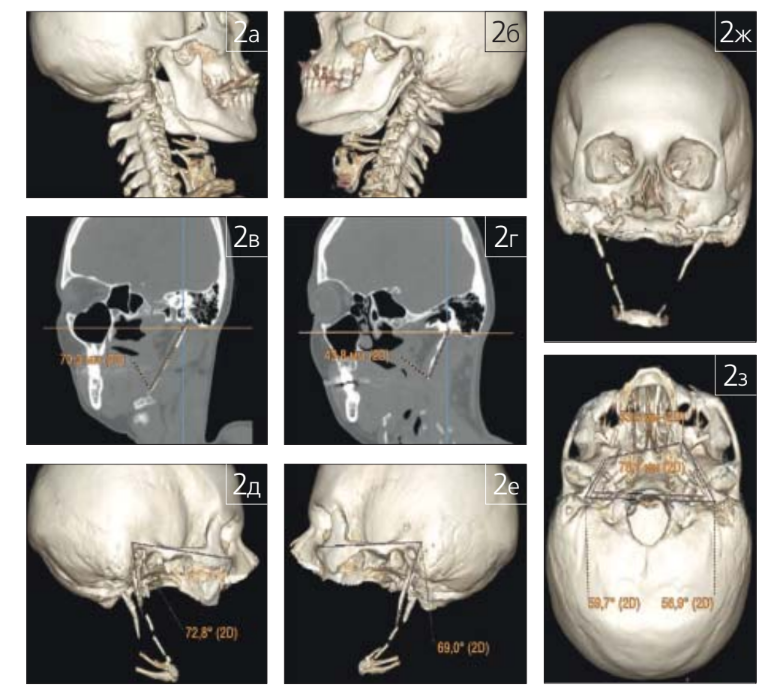
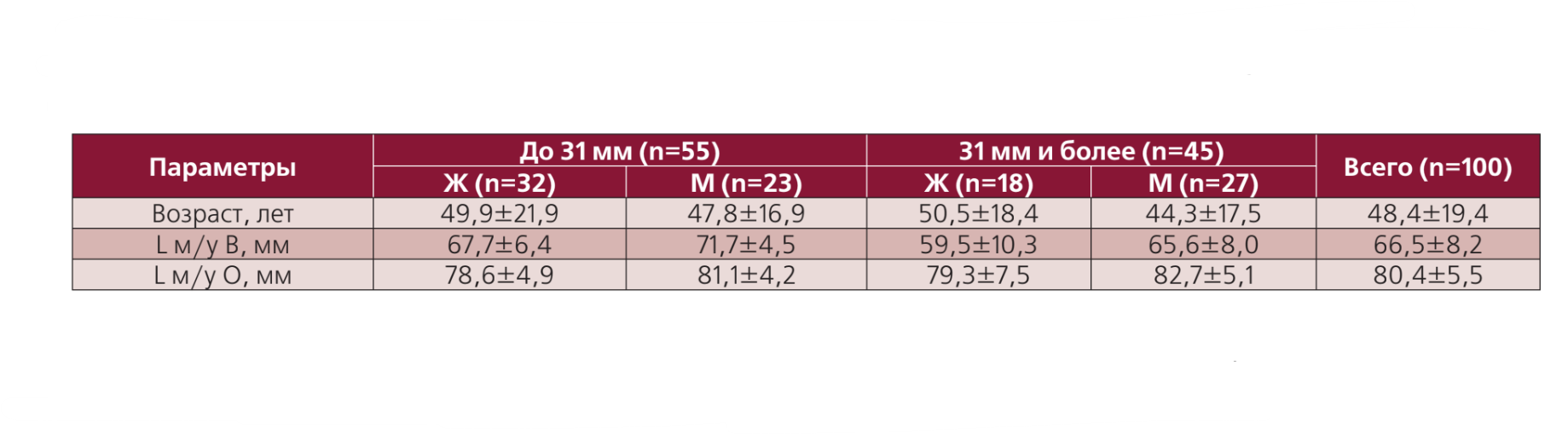
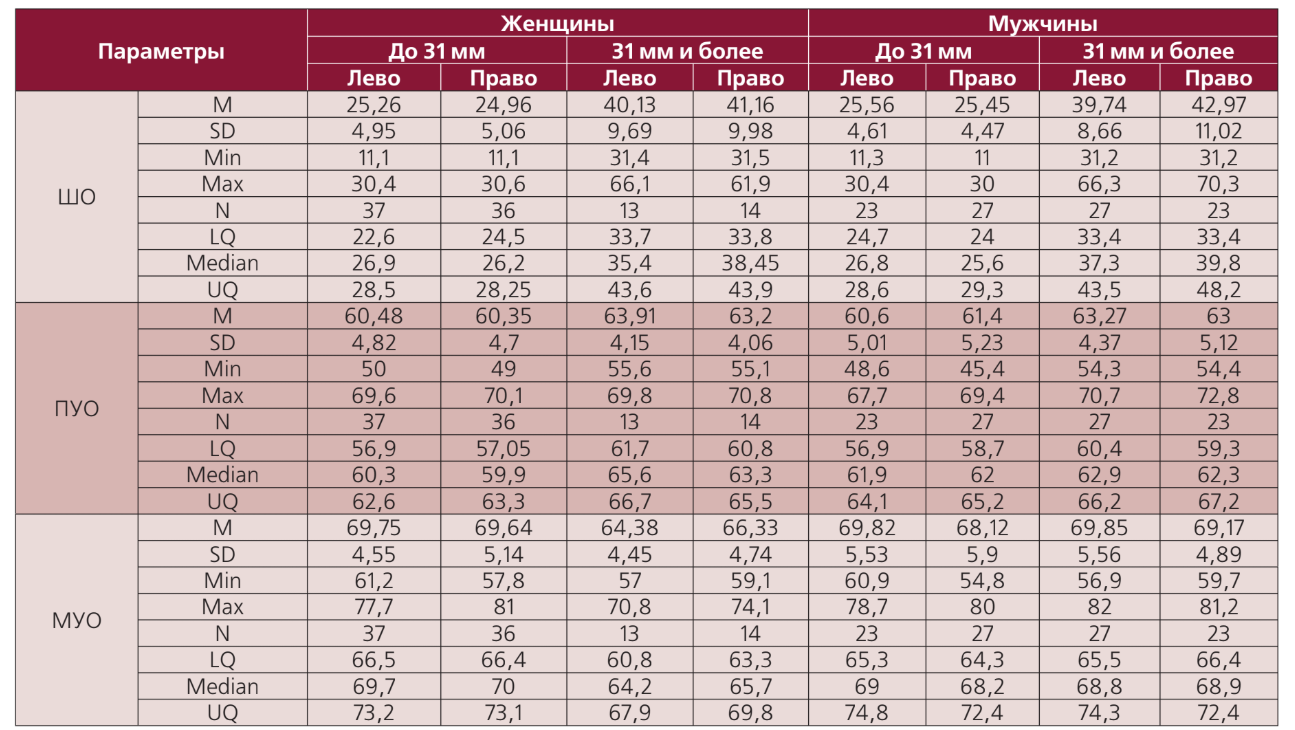
The distances between the tips and bases of the styloid processes, as well as the anterior and medial angles of deviation of the styloid processes on volumetric reconstructions based on CT data, were also evaluated. Patients were divided into groups based on the length of the styloid processes (up to 31 mm and 31 mm and above), men and women (Fig. 2, Tab. 1, 2).
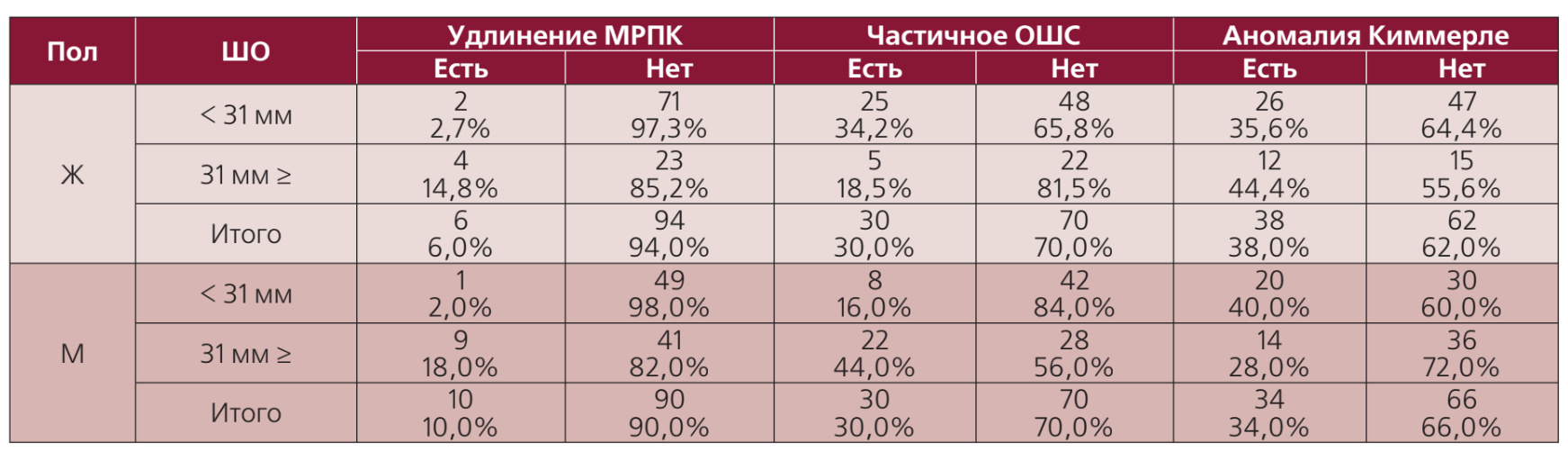
Additionally, parameters such as the presence or absence of calcifications in the stylohyoid ligaments (SHL), elongation of the lesser horns of the hyoid bone (LHHB), and the presence or absence of complete and incomplete Kimmerle anomalies were assessed (Table 2).
The diagnosis of "stylohyoid syndrome" was confirmed in 6 patients who were operated on at the clinic of maxillofacial surgery of PSPbGMU named after acad. I.P. Pavlov using endoscopically assisted surgical access. Prior to the surgical intervention, all patients underwent MSCT of the skull and cervical spine according to the examination protocol from the apex of the skull to the jugular notch of the sternum without changing the tilt angle of the center of the Gentry, intended for subsequent integration with the surgical navigation station.
Surgical technique: a linear incision was made in the hairy part of the occipital region, after incising the skin and subcutaneous adipose tissue, bundles of the sternocleidomastoid muscle fibers were visualized in the wound, and then, under the control of a rigid endoscope, dissection was performed and the sternocleidomastoid muscle was elevated with a retractor. The posterior belly of the digastric muscle was found and elevated. An electromagnetic navigation station was also used for more accurate orientation in the wound. The styloglossal fascia was then incised, and the styloid process was identified, skeletonized, and resected.
Research Results
As a result of the survey and objective examination, the following symptoms associated with the hypoglossal syndrome were identified: complaints of constant dull pain in the deep area of the face and the upper part of the lateral neck (in all patients — 100%), with radiation to the root of the tongue and pharynx (17%), to the ear area (11%), to the temporomandibular joint (66%). Pain radiation to the temporal, cheek, and submandibular areas is often noted (41%). Some patients experience pain in the teeth of the lower and upper jaws (3%). In all patients, the intensity of pain increased with wide mouth opening, talking, swallowing, and head turns and tilts. Patients also reported a sensation of a foreign body in the throat (39%). The clinical manifestations described above were unilateral in all patients who sought help. The prevalence of patients with hypoglossal syndrome in the surveyed population was 6%.
The elongation of the styloid processes was observed in 45% of cases, of which 27% were men and 18% were women, in the overwhelming majority of cases on the right side.
In the group of patients with styloid process lengths of 31 mm or more, a significant correlation was determined for parameters such as the length of the styloid process and the distance between the tips of the styloid processes (Ro= -0.45; p<0.0001), the length of the styloid process and the distance between the bases of the styloid processes (Ro=0.28; p=0.0124), the length of the styloid process and the medial angle of deviation (MAD) of the styloid process (Ro= -0.365; p=0.0011), the distance between the tips of the styloid processes and the medial angle of deviation of the styloid process (Ro=0.52675; p<0.0001), the distance between the bases and tips of the styloid processes (Ro=0.32; p=0.0042). No clear correlation of parameters with the anterior angle of deviation of the styloid process (AAD) was found (table 4).

In the group of patients with styloid process lengths less than 31 mm, a high correlation with statistical significance was determined between parameters such as the length of the styloid process and the distance between the tips of the styloid processes (Ro= -0.419; p<0.0001), the distance between the tips and the distance between the bases of the styloid processes (Ro=0.604; p<0.0001). A weak but statistically significant correlation was found between the length of the styloid processes and the anterior angle of deviation of the styloid process (Ro= -0.2063; p=0.0221), the distance between the tips of the styloid processes and the anterior angle of deviation of the styloid process (Ro=0.1987; p=0.0276), the distance between the bases of the styloid processes and the medial angle of deviation of the styloid process (Ro= -0.34; p=0.0001).
In the group of examined women, a high correlation with statistical significance was determined between the length of the styloid processes and the distance between the tips of the styloid processes (Ro= -0.6019; p<0.0001), a significant correlation between the length of the styloid processes and the medial angle of deviation of the styloid process (Ro= -0.31; p=0.0016), the distance between the bases and tips of the styloid processes (Ro=0.47; p<0.0001), the distance between the tips of the styloid processes and the medial angle of deviation of the styloid process (Ro=0.33; p=0.0008), as well as the distance between the bases of the styloid processes and the medial angle of deviation of the styloid process (Ro= -0.247; p=0.0132).
In the group of men, a high correlation with statistical significance was determined between the length of the styloid processes and the distance between the tips of the styloid processes (Ro= -0.5666; p<0.0001), as well as a correlation was determined between the distance between the bases and the tips of the styloid processes (Ro=0.299; p=0.0025), the distance between the bases of the styloid processes and the medial angle of deviation of the styloid process (Ro= -0.3257; p=0.0009), the distance between the tips of the styloid processes and the medial angle of deviation of the styloid process (Ro=0.21; p=0.032). No significant correlation was found between the length of the styloid processes and the medial angle of deviation of the styloid process in men.
Thus, with an increase in the length of the styloid process, a decrease in its medial angle of deviation is noted (p<0.05) with an increase in the anterior angle of deviation of the styloid process or without it. Compared to published data, the average length of the styloid processes in a sample of 114 individuals was 25.8 mm, with 16 individuals having a length of the styloid processes greater than 30 mm, while in their study, the average values of both the anterior and medial angles of deviation of the styloid processes decreased in the group of individuals with a length of the styloid processes greater than 30 mm.
With age, there is an increase in the length of the styloid processes and a decrease in the medial angle of deviation of the styloid process. By the age of 41-50 years, the frequency of patients with elongated styloid processes increases, and after 51 years, it decreases.
The clinical example below demonstrates the stages of examination and treatment of a patient diagnosed with "stylohyoid syndrome".
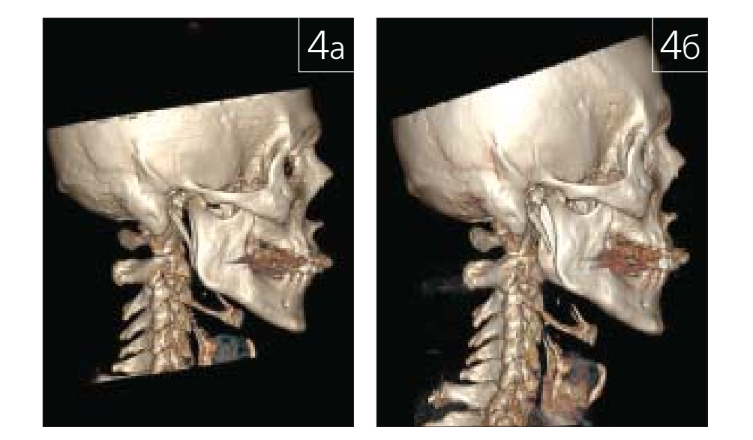
Patient N., 50 years old, presented with complaints of aching pain in the lateral area of the neck on the right, sharply increasing with wide mouth opening, swallowing, radiating to the right ear and the temporal region on the right. From the history, it is known that the pain first occurred a year ago after an exacerbation of chronic tonsillitis. At the examination stage, the patient was consulted by an otorhinolaryngologist and a neurologist, and a CT scan of the skull and cervical spine was performed according to the examination protocol. Upon admission, a repeat pharyngoscopy was performed: the throat was symmetrical, the mucous membrane of the oropharynx showed no acute inflammatory changes at the time of examination, the palatine tonsils were atrophic, the lacunae were clean, and there were no deposits. Upon palpation of the tonsillar fossa on the right, a hard fragment with clear mesio-distal borders was found, contouring under the mucous membrane of the tonsillar fossa. The surgical intervention was performed using the method described above: endoscopically assisted resection of the right styloid process of the temporal bone under the control of an electromagnetic navigation station. Figure 3 shows a screenshot from the navigation surgical station and an endoscopic view of the surgical wound. Figure 4 presents volumetric reconstructions of the patient's CT scan before and after the operation.


In the early postoperative period, the patient noted the absence of pain and difficulties in swallowing and opening the mouth. The healing of the wound in the occipital area occurred with primary tension without signs of inflammation. Fig. 5 shows the pharyngoscopy and the extent of the patient's mouth opening on the 3rd day after the surgery. Fig. 6 presents photographs of the patient before and on the 3rd day after the surgery.


The patient was discharged on the 4th day after the surgery.
The stitches were removed on the 14th day after the surgery.
Conclusion
Thus, the proposed volume of examination for patients allows for consideration of all clinical and radiological features of the course of the disease "stylohyoid syndrome".
Qualitative and quantitative analysis of MSCT of the facial skull and cervical spine with post-processing of the images allows for the confirmation of the diagnosis "stylohyoid syndrome" to determine the volume and tactics of treatment for patients, as well as to select the optimal surgical access.
The proposed endoscopically assisted surgical access is one of the methods of choice for the surgical treatment tactics of stylohyoid syndrome; its application allows for improved functional and cosmetic results of the surgical intervention and reduces the duration of postoperative rehabilitation for patients.
A.I. Yaremenko, A.A. Zubareva, O.V. Lukina, S.A. Karpishchenko, T.E. Kolegova, M.V. Malyarevskaya
References
Karlov V.A. Face neurology. - M., Medicine, 1991. - P. 285.
Lebedyancev V.V. Stylohyoid syndrome: topographic-anatomical foundations, clinic, diagnosis, treatment principles: author's abstract of the dissertation for the degree of Doctor of Medical Sciences: 14.00.21, 14.00.02 / Central Scientific Research Institute of Dentistry of the Ministry of Health of the Russian Federation. - Moscow, 2004. - 44 p.
Shevryigin B.V., Mchelidze G.P. Handbook of Otorhinolaryngology. - M., TOO Triada-X. - 1998. - P. 448.
Shulga I.A., Lebedyantsev V.V., Kagan I.I., Zaitsev N.V., Uksukbaeva N.V. Factors of pathogenesis of stylohyoid syndrome // Russian otorhinolaryngology. - 2011. - Vol. 53, No. 4. - P. 175-182.
Dou G., Zhang Y., Zong C., Chen Y., Guo Y., Tian L. Application of surgical navigation in styloidectomy for treating Eagle’s syndrome // Ther Clin Risk Manag. - 2016. - No. 12. - P. 575-83.
Ghosh L.M., Dubey S.P. The syndrome of elongated styloid process // Auris Nasus Larynx. - 1999. - No. 26 (2). - P. 169-175.
Matsumoto F., Kase K., Kasai M., Komatsu H., Okizaki T., Ikeda K. Endoscopy-assisted transoral resection of the styloid process in Eagle’s syndrome. Case report // Head Face Med. - 2012. - No. 8. - P. 21-24.
Muderris T., Bercin S., Sevil E., Beton S., Kırıs M. Surgical management of elongated styloid process: intraoral or transcervical? // Eur Arch Oto-rhinolaryngol. - 2014. - No. 271(6). - P. 1709-1713.
Sachin Patil et al. Morphometric Study of the Styloid Process of Temporal Bone. Journal of Clinical and Diagnostic Research. - 2014. - Vol-8(9): AC04-AC06.
Werhun E.L., Weidenhaft M.C., Palacios E., Neitzschman H. Stylohyoid syndrome, also known as Eagle syndrome: an uncommon cause of facial pain // Ear Nose Throat J. - 2014. - No. 93 (9). - P. 384-385.