
Identification of Prognostic Factors for Sialadenitis Development in Patients Undergoing Radioiodine Therapy
Machine translation
Original article is written in RU language (link to read it) .
Introduction. Radioiodine therapy is a modern method for treating thyroid gland pathology. Its application is possible both in malignant formations and in thyrotoxicosis. However, this technique has a complication in the form of impaired salivary gland function, which causes dryness in the oral cavity, its enlargement, and pain syndrome. The aim of our study was to identify risk factors for the development of functional disorders of the salivary glands in patients who underwent radioiodine therapy.
Materials and methods. A retrospective open two-center non-randomized study was conducted, which included 61 patients who received radioiodine therapy for thyroid diseases. In 33/61 patients, signs of sialadenitis development against the background of and after radioiodine therapy were not registered. In twenty-eight patients (28/61), salivary gland damage was detected against the background of the therapy. A statistical analysis of data on gender, age, primary clinical diagnosis, stage of the primary disease, dose of I131 received, presence or absence of sialadenitis, and the time of sialadenitis development was conducted.
Results. The analysis of the obtained data revealed that independent adverse factors increasing the risk of salivary gland damage in patients who received at least one session of radioiodine therapy were: female gender (p=0.0219; OR 10.38: 95% CI 1.40–76.84) and age 61 years and younger (p = 0.0004; OR 1.04: 95% CI 1.02–1.06). The median cumulative dose of the radiopharmaceutical did not show significance in the multifactorial analysis.
Conclusion. The development of chronic sialadenitis against the background of radioiodine therapy is a multifactorial pathology. This pathology requires dynamic observation and preventive measures, especially for the risk group (female gender and age 61 years and younger).
Introduction
Radioiodine therapy is one of the treatments for thyroid gland pathology. This method is based on the understanding of the mechanisms of I131 transport from the blood via the Na-I-symporter into the follicular epithelium of the thyroid gland. However, during this treatment, it is possible to disrupt the function of the salivary glands due to the same mechanisms and the physiological accumulation of the radiopharmaceutical in them. The incidence of chronic sialadenitis after I131 therapy reaches up to 67%.
Loss of salivary gland function and the formation of pain syndrome affects the quality of life of patients and can lead to disruptions in their social life.
Persistent dry mouth complicates the formation of a food bolus and speech, and also contributes to the development of pathological changes in the oral mucosa and damage to the hard tissues of the teeth.
Currently, there are only a few studies analyzing the risk factors for the development of salivary gland pathology. The articles discuss indicators such as cumulative dose, gender, age, and even nationality; some studies focus solely on subjective patient indicators, such as dry mouth. However, methods for preventing this complication have not yet been identified. The use of amifostine, selenium, vitamins A and E, salivary-stimulating diets, and massage of the salivary glands is recommended. Data on the effectiveness of these methods, options for their use, as well as the dependence of salivary gland dysfunction development on the dose of the administered drug, are contradictory.
Therefore, the aim of our study was to identify possible prognostic risk factors for the development of sialadenitis in patients who received radioiodine therapy for thyroid diseases.
Materials and Methods
A retrospective open two-center non-randomized study was conducted, which included a total of 61 patients. All patients received radioiodine therapy for thyroid diseases in the department of radiosurgical treatment with open radionuclides of the A.F. Tsyba Medical Radiological Scientific Center – a branch of the Federal State Budgetary Institution "NMITs Radiology" of the Ministry of Health of Russia from 2000 to 2022. In 33/61 patients, no signs of sialadenitis development were recorded against the background of and after radioiodine therapy. Twenty-eight patients (28/61), who were found to have salivary gland lesions during the therapy, were referred to the clinic of maxillofacial surgery of the Federal State Budgetary Educational Institution of Higher Education "Pavlov First Saint Petersburg State Medical University" of the Ministry of Health of Russia for salivary gland lesions after radioiodine therapy from 2017 to 2022. For further analysis, all patients were divided into two groups depending on the presence or absence of clinical signs of salivary gland lesions. Patients in group 1 (main; 28 patients) had signs of salivary gland lesions, while patients in group 2 (control; 33 patients) had no salivary gland lesions.
Patients underwent a standard examination (complaints, medical history and life history, palpation of the salivary glands, oral cavity examination), scintigraphy to assess the accumulation of radiopharmaceuticals in the salivary glands.
In the presence of clinical signs of salivary gland pathology, an ultrasound examination of the salivary glands and lymphatic system of the head and neck was initially performed, as well as sialendoscopy of the ducts of the salivary gland system to determine functional disorders of the salivary glands.
The variables studied included gender, age, primary clinical diagnosis, stage of the underlying disease, dose of I131 received, presence or absence of sialadenitis, and the time from the start of radionuclide therapy to the development of sialadenitis.
The main inclusion criteria for patients in the study were:
The ability and consent to sign a voluntary informed consent form to participate in the study.
Patient age – over 18 years.
Conducting radioiodine therapy for thyroid diseases.
The main criteria for excluding patients from the study were:
Registered presence of any comorbid conditions in the stage of subcompensation and decompensation.
Presence of salivary gland diseases prior to radioiodine therapy.
Presence of any adverse events after radionuclide treatment that did not resolve to grade 1 toxicity, as determined by the CTCAE ver. 5.0 scale (except for salivary gland damage).
At the first stage of statistical analysis, the normality of distribution of quantitative variables was checked using the Shapiro-Wilk test. In cases where the data followed a normal distribution, descriptive statistics of the variables were performed using the mean and standard deviation (M±SD), while in cases where the data did not follow a normal distribution, the median and interquartile range (Me [Q25–Q75]) were used.
Comparison of numerical variables with a normal distribution was carried out using Student's t-test; in the case of deviation from normal distribution, comparison of independent variables was performed using the Mann-Whitney test, and comparison of dependent variables was conducted using the Wilcoxon test.
Comparison of large groups of patients by the frequency of occurrence of a nominal feature was conducted using the z-test (with Yates' continuity correction), χ2 test (with Yates' continuity correction); comparison of small groups of patients (5 or fewer) was performed using Fisher's exact test.
To determine the prognostic value of the factors under consideration, ROC analysis was conducted with the construction of ROC curves, calculation of the area under the curve (AUC), and determination of the sensitivity level (the proportion of true positive cases) and specificity (the proportion of true negative cases). Using ROC analysis, the optimal threshold value for each of the studied indicators ("cut-off point") was determined; the optimality of the chosen threshold value was assessed using Youden’s J index.
The analysis of the development of salivary gland lesions against the background of RYT was conducted using the Kaplan-Meier procedure. The comparison of event development curves was performed using the log-rank test, as well as by constructing a Cox regression model using the backward elimination method (depending on the chosen statistical model).
Statistical data processing was carried out using the STATISTICA® (StatSoft, ver. 12.0) application statistical software package, the MedCalc® (ver. 20.118) statistical software package, and Microsoft® Excel (ver. 16.16.12).
Research Results
Initially, an analysis of the general characteristics of the patients was conducted. Group 1 consisted of 3.57% men and 96.43% women, aged from 21 to 77 years, with a mean age of 59.54±13.75 years (95% CI 45.20–55.87). Group 2 consisted of 39.39% men and 60.61% women, aged from 26 to 82 years, with a median age of 68 years [59.75–75.00]. There were significantly more women in group 1 than in the control group (p = 0.0010), and all patients in group 1 were significantly younger than patients in group 2 (control) (p = 0.0001).
When analyzing the total dose of radiopharmaceutical received during the treatment of the first group of patients, the median dose after which patients in this group developed salivary gland damage was 3.86 GBq [3.50–4.00] (while the total cumulative dose ranged from 2.56 to 6.77 GBq), which was significantly lower than in the control group – p < 0.0001.
The total cumulative dose received during the treatment of patients in the control group was significantly higher, ranging from 37.00 to 100.00 GBq, and the median dose received was 51.90 GBq [42.80–74.00] without signs of salivary gland damage.
ROC analysis revealed significant models when determining the influence on the risk of developing salivary gland damage against the background of or after radioiodine therapy, considering the patients' gender, their age, and the total received dose (GBq) (see figure).
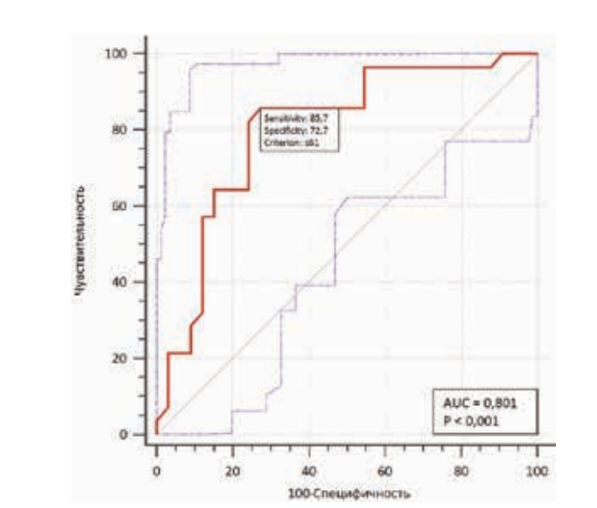
Based on the threshold values of each of the examined indicators identified through the ROC analysis, a univariate analysis was conducted to assess their impact on the risk of salivary gland damage in patients during or after radioiodine therapy.
Without considering the influence of each other, all analyzed indicators had a statistically significant impact on the risk of salivary gland damage in patients during or after radioiodine therapy: gender, age, and total dose of radioiodine therapy.
However, in order to determine the true prognostic value of the examined factors on the development of salivary gland damage in patients, all significant parameters were included in a multivariate Cox proportional hazards model (see table). The model assessing the impact of the examined factors on the timing of salivary gland damage after at least one session of radioiodine therapy included the following indicators: gender, age of patients with a threshold value not exceeding 61 years, and total accumulated dose of radioiodine therapy with a threshold value not exceeding 6.77 GBq. Overall, the constructed model was statistically significant: p<0.0001, and the quality of the constructed model was good.
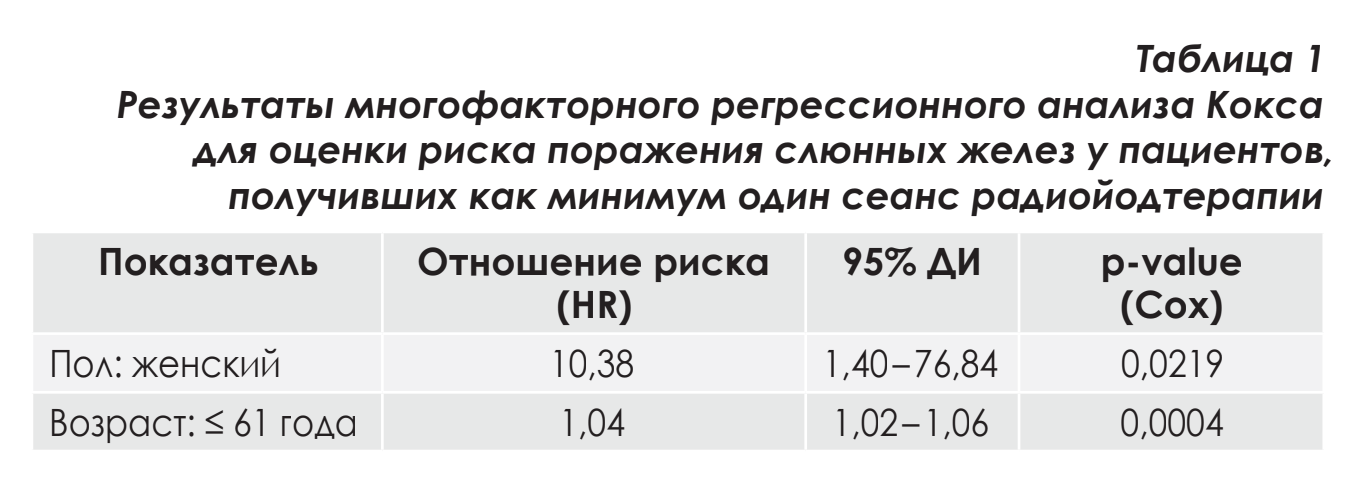
The multifactorial analysis conducted allowed us to establish that the independent factors with a statistically significant negative impact on the risk of developing salivary gland lesions in patients who received at least one session of radioiodine therapy were female gender and age 61 years or younger.
Discussion
The development of salivary gland dysfunction during radioactive iodine ablation is a relevant issue for patients, as they are of working age, lead active social lives, and have long survival times. Currently, there is no clear algorithm for the prevention and treatment of this pathology, so identifying risk factors may be a link in developing a prevention algorithm for this complication. Salivary gland damage can be acute or develop over time, even after a single administration of the drug [10, 11, 12]. When analyzing factors without mutual influence, it was found that salivary gland disorders are possible at doses greater than 3.86 GBq. This is confirmed by studies from various authors who assessed salivary gland function under scintigraphy conditions. Several authors noted that at a dose of 3.7 GBq or less, a possible limiting factor for salivary gland damage was the activation of their internal compensatory mechanisms. Since the therapeutic dose of I131 is calculated individually for each patient and depends on the volume of the thyroid gland, the type and stage of the underlying disease, it can be said that administering a dose above 3.86 GBq should alert practicing doctors, and within the framework of the algorithm for identifying adverse events, additional studies of the salivary glands should be conducted.
When analyzing the literature sources, it was found that most studies focused only on one factor regardless of others, and some authors studied patients with already developed xerostomia before the introduction of radiopharmaceuticals: for example, xerostomia that was registered only based on the subjective feelings of the patient [4, 5, 6]. In our study, we conducted a multifactorial analysis, which showed that the true risk factors may be female gender and age of 61 years and younger.
Conclusion
Thus, the obtained results indicate that women aged 61 years and younger are more susceptible to the development of sialadenitis against the background of radioiodine therapy. Therefore, it is necessary to distinguish such patients into a separate group with an increased risk factor for complications and to conduct additional types of analyses in the form of dynamic scintigraphy and ultrasound examination of the salivary glands at the pre-hospital stage to assess the primary status of the patient. The median total accumulated dose of radioiodine therapy, after which the development of salivary gland damage in this group is possible, was 3.86 GBq [3.50–4.00], which, although it did not show significance in the multifactorial analysis, increased the risk of developing sialadenitis in the unifactorial analysis.
Dynamic monitoring is also necessary to minimize the development of obstructive pathology of the salivary glands, as well as the performance of sialendoscopy to reduce the formation of duct structures.
A.Ya. Razumova, S.I. Kutukova, A.I. Yaremenko, E.V. Borodavina, N.L. Petrov
References
Garbuzov P.I., Drozdovskij B.I., Rodichev A.A. et al. Radioiodine therapy for thyroid cancer. Practical Oncology. 2007; 1(29):42–45. Garbuzov P.I., Drozdovskij B.I., Rodichev A.A. et al. Radioiodine therapy for thyroid cancer. Practical Oncology. (In Russ) 2007; 1(29):42–45.
Danilova L.I., Valuyevich V.V. Radioiodine therapy for benign thyroid diseases. Problems of Endocrinology. 2006;52(2):43–47. https://doi.org/10.14341/probl200652243-47. Danilova L.I., Valuyevich V.V. Radioiodine therapy for benign thyroid diseases. Problems of Endocrinology. 2006;52(2):43-47. (In Russ.)https://doi.org/10.14341/probl200652243-47.
Krčálová E., Horáček J., Gabalec F., Žák P., Doležal J. Scintigraphic evaluation of salivary gland function in thyroid cancer patients after radioiodine remnant ablation. Eur J Oral Sci. 2020;128(3):204-210. https://doi.org/: 10.1111/eos.12689
Hollingsworth B., Senter L., Zhang X., Brock G.N., Jarjour W., Nagy R., Brock P., et al. Risk Factors of 131I-Induced Salivary Gland Damage in Thyroid Cancer Patients. J Clin Endocrinol Metab. 2016;101(11):4085-4093. doi: 10.1210/jc.2016-1605.
Riachy R., Ghazal N., Haidar M.B., Elamine A., Nasrallah M.P. Early Sialadenitis After Radioactive Iodine Therapy for Differentiated Thyroid Cancer: Prevalence and Predictors. Int J Endocrinol. 2020;2020:8649794. doi: 10.1155/2020/8649794.
Sánchez Barrueco A., González Galán F., Alcalá Rueda I., Santillán Coello J.M., Barrio Dorado M.P., Villacampa Aubá J.M., Escanciano Escanciano M. et al. Incidence and risk factors for radioactive iodine-induced sialadenitis. Acta Otolaryngol. 2020;140(11):959-962. doi: 10.1080/00016489.2020.1802507.
Jentzen W, Richter M, Nagarajah J, Poeppel TD, Brandau W, Dawes C, Bockisch A, Binse I. Chewing-gum stimulation did not reduce the absorbed dose to salivary glands during radioiodine treatment of thyroid cancer as inferred from pre-therapy (124)I PET/CT imaging. EJNMMI Physics 2014; 1: 100. doi: 10.1186/s40658-014-0100-1.
Auttara-Atthakorn A., Sungmala J., Anothaisintawee T., Reutrakul S., Sriphrapradang C. Prevention of salivary gland dysfunction in patients treated with radio-iodine for differentiated thyroid cancer: A systematic review of randomized controlled trials. Front Endocrinol (Lausanne). 2022;13:960265. https://doi.org/10.3389/fendo.2022.960265.
Ahn B.C. Reduction of Salivary Gland Damage During Radioiodine Therapy for Differentiated Thyroid Cancers. Nucl Med Mol Imaging. 2020 Jun;54(3):126–127. https://doi.org/10.1007/s13139-020-00643-w.
Baudin C., Bressand A., Buffet C., Menegaux F., Soret M., et al. Dysfunction of the Salivary and Lacrimal Glands After Radioiodine Therapy for Thyroid Cancer: Results of the START Study After 6-Months of Follow-Up. Thyroid. 2023;33(9):1100-1109. https://doi.org/10.1089/thy.2023.0090.
Upadhyaya A., Meng Z., Peng W., Guizhi Z., et al. Effects of first radioiodine ablation on functions of salivary glands in patients with differentiated thyroid cancer. Medicine. 2017; 96(25):p e7164. https://doi.org/10.1097/MD.0000000000007164
An YS, Yoon JK, Lee SJ, Song HS, Yoon SH, Jo KS. Symptomatic late-onset sialadenitis after radioiodine therapy in thyroid cancer. Ann Nucl Med. 2013;27(4):386-91. https://doi.org/10.1007/s12149-013-0697-5.
Horvath E., Skoknic V., Majlis S., Tala H., Silva C. et al. Radioiodine-Induced Salivary Gland Damage Detected by Ultrasonography in Patients Treated for Papillary Thyroid Cancer: Radioactive Iodine Activity and Risk. Thyroid. 2020 Nov;30(11):1646-1655. doi: 10.1089/thy.2019.0563.