
Intraductal Surgery of Salivary Glands in Patients After Radioiodine Therapy
Machine translation
Original article is written in RU language (link to read it) .
Objective — to describe and evaluate the methods of diagnosis and treatment of sialadenitis that developed after radioiodine therapy.
Materials and methods. Diagnosis and treatment were conducted for 28 patients diagnosed with "Chronic sialadenitis or exacerbation of chronic sialadenitis." The diagnosis included a questionnaire, examination, probing, ultrasound examination with an extraoral sensor, without stimulation of saliva production, and diagnostic sialoendoscopy. In the presence of obstructive pathology of the ductal system, therapeutic sialoendoscopy was performed.
Results. Clinical symptoms could affect various salivary glands, with the parotid glands being most commonly affected bilaterally (36%), and primary manifestations according to the history were observed within a period of 6 months to a year (35%). Structural changes in at least one salivary gland were present in 16 out of 28 patients (57%). During ultrasound visualization of ductal dilation during sialoendoscopy, a single stricture of the duct was identified in 15 out of 28 cases (54%). During sialoendoscopy, obstructive changes in the ductal system were represented by mucous plaques, stenoses, and strictures, which could be single, multiple, or total narrowing. When ductal obstruction was detected, it was eliminated, restoring ductal patency.
Conclusion. Given the development of minimally invasive technologies and the increased sensitivity of ultrasound examination, further study of this topic is necessary.
Introduction
Radioiodine therapy is a widely used method for treating thyroid diseases, especially in cases of malignant neoplasms. The goal of treatment is to remove the remaining thyroid tissue after thyroidectomy. I131 molecules accumulate in altered thyrocytes, ultimately leading to their destruction. In the presence of malignant tumors in the thyroid gland, radioiodine therapy becomes a necessary procedure that significantly improves the prognosis of the disease. Although this method has certain advantages, it is also associated with the risk of complications.
In addition to the thyroid gland, numerous tissues and organs in the human body have the ability to accumulate radioactive iodine. These include salivary glands, the mucosa of the gastrointestinal tract, gonads, and mammary glands during lactation. The incorporation of I131 into cells is mediated by the sodium-iodide symporter. Due to the ability of the salivary gland to accumulate iodine, changes in the parenchyma may occur, leading to hypofunction, xerostomia, dysphagia, and sialadenitis.
The parotid salivary gland (PSG) is more susceptible to radiation exposure than the submandibular gland (SMG), as it mainly consists of serous cells, which are more sensitive to radiation than other salivary gland cells. As a result, parotid glands are affected more frequently than sublingual and submandibular glands. After radioiodine therapy, patients may complain of pain and swelling in the parotid area, hyposalivation, as well as enlargement of the salivary glands at different times.
The methods for diagnosing this complication can vary. Ultrasound diagnostics are commonly used to identify the characteristics of stenosis, duct dilation, kinking, megaduct, and echogenicity. Sialoendoscopy is used to assess the diameter of stenosed and normal ducts, the location of the narrowing, the length of the duct, and the type of tissue in the affected area. When conducting scintigraphy, the authors identified a borderline dose activity of 5.55 GBq, beyond which a decrease in saliva production is observed.
At present, there is no established algorithm for the treatment of salivary glands after radioiodine therapy in the available literature. Only attempts are being made to study the use of massage, parasympathetic stimulation (pilocarpine), hypnosis, gene therapy, protective protein injections, and sialoendoscopy as methods for dilating small strictures and irrigating the ducts of the salivary glands.
The aim of our study is to describe and evaluate the methods of diagnosis and treatment of sialoadenitis that developed after radioiodine therapy.
Materials and Methods
Treatment was conducted for 28 patients diagnosed with chronic sialoadenitis or exacerbation of chronic sialoadenitis at the oncology department No. 8 (CHLH) of the Federal State Budgetary Educational Institution of Higher Education "Pavlov First Saint Petersburg State Medical University".
All medical studies comply with the Helsinki Declaration on medical protocols. Informed consent was obtained from all participants.
Descriptive statistics methods were used to describe the variables reflecting the characteristics. At the first stage of statistical analysis, the normality of distribution of quantitative variables was checked using the Shapiro-Wilk test. In cases where the data followed a normal distribution, descriptive statistics of the variables were performed using the mean and standard deviation (M±SD), while for data that did not follow a normal distribution, the median and interquartile range (Me [Q25–Q75]) were used. Statistical data processing was carried out using the MedCalc® (ver. 20.118) application statistical software package and Microsoft® Excel (ver. 16.16.12).
Among the 28 patients, there were 27 women (95.26%) and 1 man (4.74%). The age of the patients ranged from 21 to 77 years, with a mean age of 50.54±13.75 years (95% CI 45.20–55.87). The general inclusion criteria for patients in the study:
Patients must be informed and give voluntary written consent to participate in the clinical study.
Patients were admitted to the clinic on an emergency or planned basis with a diagnosis of: exacerbation of chronic / chronic sialadenitis.
Patients have a history of treatment with radioactive iodine.
All patients were required to undergo a comprehensive examination.
All patients were indicated for therapeutic measures. Patients with pre-existing salivary gland diseases were excluded. A standard clinical examination (interview, examination, probing) was conducted, as well as an ultrasound examination using a device (SonoScape S8Exp, China) with an extraoral sensor, without stimulating saliva production. Diagnostic sialoendoscopy was performed using a semi-rigid endoscope (Karl Stortz, Germany) with diameters of 1.1 and 1.6 mm.
During the visualization of one or multiple strictures or stenoses, therapeutic sialoendoscopy was immediately performed using ductal orifice dilators, bougies, drills of various diameters, and catheters.
Results and Discussion
Physiological iodine absorption mediated by the sodium-iodine symporter in the salivary gland makes it susceptible to damage caused by radioactive iodine, which can lead to the development of inflammatory processes and xerostomia.
Primary data play an important role in the diagnosis and treatment of this pathology. By analyzing this data, it is possible to identify the characteristics of clinical manifestations. In 25 out of 28 cases (89.29%), patients received radioiodine therapy for malignant thyroid neoplasms, and only in 3 cases (10.71%) — for other pathologies, such as diffuse toxic goiter. The minimum activity of the administered radiopharmaceutical was 2.56 GBq, while the maximum was 5.82 GBq, with a median total dose of 3.86 GBq [3.50–4.00], and the procedure was performed twice for two patients out of 28 (7%).
Clinical symptoms could be identified in different salivary glands, and the damage could be unilateral or bilateral (Table 1), as well as manifesting at different times. No lesions of the OSJ and PSJ were detected on one side. The main complaints were swelling of the salivary gland (Fig. 1), pain, a feeling of heaviness, and dryness in the oral cavity. All patients (n=28) were divided according to the timing of the onset of primary symptoms of damage to the major salivary glands:
• Group 1, 8 (28.57%) — up to 6 months;
• Group 2, 10 (35.71%) — from 6 months to 1 year;
• Group 3, 6 (21.44%) — from 1 year to 2 years;
• Group 4, 4 (14.28%) — later than 2 years. The median time from the start of radioiodine ablation (the first course of radioiodine therapy) to the development of salivary gland damage was 14.5 months (95% CI 11.0–113.0).


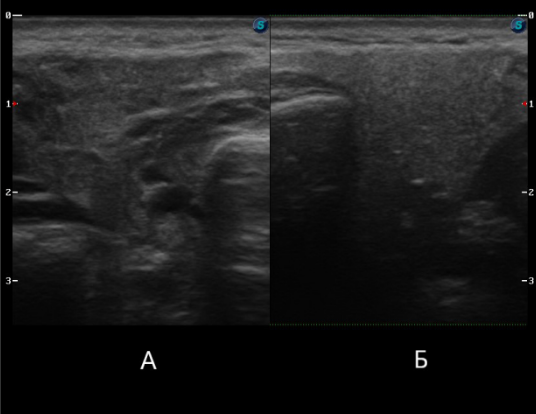
All patients (n=28) underwent ultrasound examination of all major salivary glands. Various changes were visualized: decreased echogenicity, structural heterogeneity, duct dilation, lymphadenopathy (Fig. 2). When assessing the condition of the salivary glands, it was found that their involvement could vary from at least one gland to all, as well as the number of changes. For example, one patient could have structural disruption of the parotid salivary gland and dilation of the submandibular salivary gland duct. However, no patient with isolated damage to the sublingual salivary gland was identified. In analyzing the data, we did not find a pattern in the severity of pathological changes or the number of affected salivary glands in relation to the activity of the radiopharmaceutical. However, in the study by E. Horvath et al., it was found that the highest frequency of possible damage (77.7%) to the salivary glands may be associated with the activity of I131 7400 MBq.
Structural changes were present in at least one salivary gland in 16 out of 28 patients (57%).
All (n=28) underwent diagnostic sialoendoscopy. The number of examined salivary glands depended on the presence of complaints. A total of 35 parotid glands and 14 submandibular glands were examined (Table 2).

It was also found that during ultrasound visualization of duct dilation during sialoendoscopy, a single stricture of the duct of the parotid or submandibular salivary gland was identified in 15 out of 28 cases (54%).
In the visualization of single and multiple strictures, in all cases, their excision was performed using a drill, as well as the placement of a catheter to prevent the recurrence of stricture formation. In cases of total stricture of the duct system, only symptomatic therapy aimed at reducing the frequency of inflammatory processes in the salivary gland was prescribed.
Conclusion
To date, the diagnosis and treatment of salivary gland pathology after radioiodine therapy does not have a clear algorithm. Visual criteria for the damage to the duct system, which could justify the choice of treatment method and its prognostic success, have not been developed. Therefore, this topic remains relevant and requires further study.
Funding of the study and conflict of interest. The study was not funded by any source, and there are no conflicts of interest related to this research.
A. I. Yaremenko, A. Ya. Razumova, N. L. Petrov, S. I. Kutukova, A. L. Vaaz
Literature
Bichev R. O., Gayduk I. V., Panin A. M., Mkrtumyan A. M., Vartanyan K. F., Kirienko S. L., Mirzoyants S. G. Sialadenitis during therapy with radioactive iodine-131. (Review of the literature. A case report). Rossiiskaya stomatologiya 2015; 8(4): 19–24, https://doi.org/10.17116/rosstomat20158419–24.
Kovalenko V.A., Kopchak A.V., Kovalenko A.E. Postradial sialozoadenitis in patients with papillary carcinoma of the thyroid gland. Vestnik khirurgii im. I.I. Grekova 2015; 174(1): 75–77, https://doi.org/10.24884/0042–4625–2015–174–1–75–77.
Tavares C., Coelho M. J., Eloy C., Melo M., da Rocha A. G., Pestana A., Batista R., Ferreira L. B., Rios E., Selmi-Ruby S., Cavadas B., Pereira L., Sobrinho Simoes M., Soares P. NIS expression in thyroid tumors, relation with prognosis clinicopathological and molecular features. Endocr Connect 2018; 7(1): 78–90, https://doi. org/10.1530/EC-17–0302.
Krcalova E., Horacek J., Gabalec F., Zak P., Dolezal J. Scintigraphic evaluation of salivary gland function in thyroid cancer patients after radioiodine remnant ablation. Eur J Oral Sci 2020; 128(3): 204–210, https://doi.org/10.1111/eos.12689.
Stephens L.C., Schultheiss T.E., Price R.E., Ang K.K., Peters L.J. Radiation apoptosis of serous acinar cells of salivary and lacrimal glands. Cancer 1991; 67(6): 1539–1543, https://doi.org/10.1002/1097–0142(19910315)67:6<1539:: aid-cncr2820670613>3.0.co;2-q.
Abok K., Brunk U., Jung B., Ericsson J. Morphologic and histochemical studies on the differing radiosensitivity of ductular and acinar cells of the rat submandibular gland. Virchows Arch B Cell Pathol Incl Mol Pathol 1984; 45(4): 443–460, https://doi.org/10.1007/BF02889885.
Goncalves M., Mantsopoulos K., Schapher M., Iro H., Koch M. Ultrasound in the assessment of parotid duct stenosis. J Ultrasound Med 2019; 38(11): 2935–2943, https://doi.org/10.1002/jum.14999.
Krcalova E., Horacek J., Gabalec F., Zak P., Dolezal J. Salivary gland function in thyroid cancer patients with radioiodine administration history. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub 2020; 164(3): 277–283, https://doi.org/10.5507/bp.2019.023.
Pascoe C., Duncan C., Lamb B. W., Davis N. F., Lynch T. H., Murphy D. G., Lawrentschuk N. Current management of radiation cystitis: a review and practical guide to clinical management. BJU Int 2019; 123(4): 585–594, https://doi.org/10.1111/bju.14516.
Horvath E., Skoknic V., Majlis S., Tala H., Silva C., Castillo E., Whittle C., Niedmann J. P., Gonzalez P. Radioiodine-induced salivary gland damage detected by ultrasonography in patients treated for papillary thyroid cancer: radioactive iodine activity and risk. Thyroid 2020; 30(11): 1646–1655, https://doi.org/10.1089/thy.2019.0563.