
Bone Regeneration Biomarkers in Maxillofacial Surgery: A Critical Literature Review
Machine translation
Original article is written in RU language (link to read it) .
Summary
Relevance. It is known that when drug-associated osteonecrosis occurs, a number of pathological changes arise. The titers of biomarkers responsible for bone tissue metabolism are also subject to these changes. They are important in the diagnosis and treatment planning of patients, especially during surgical interventions, due to the risk of osteonecrosis. The aim is to identify markers of bone remodeling and endothelial disruption that are most significant for optimizing the early diagnosis of microcirculation disorders in patients with maxillofacial pathologies based on data from modern scientific literature and articles.
Materials and methods. A review of the available data in the literature on normal bone anatomy, bone tissue biomarkers, and regulatory factors. Study of diagnostic regimes and identification of the most valuable and rapid indicators of bone and endothelial vessel disruption.
Results. According to the research, osteocalcin, C-terminal telopeptide, and tartrate-resistant acid phosphatase, VEGF are the most informative in clinical practice for predicting the occurrence of osteonecrosis of the jaw bones. When the concentration of C-terminal telopeptide in serum is less than 100 pg/mL, the risk of osteonecrosis increases. Serum osteocalcin is considered a specific biomarker of osteoblast function for assessing the rate of bone tissue formation in osteoporosis. The average level of osteocalcin showed a significant difference between postmenopausal osteoporosis (16.16 ± 4.5 ng/mL) and non-osteoporotic (11.26 ± 3.07 ng/mL) in women. Tartrate-resistant acid phosphatase (TRAP 5b) is used as a standard for the activity and quantity of osteoclasts. TRAP 5b can be specifically detected in serum using immunoassays.
Conclusion. The study of bone tissue degeneration markers and vascular markers allows for a clearer understanding of the principles of osteonecrosis development and, consequently, a more accurate prediction and diagnosis of osteonecrosis, as well as the appropriate selection of treatment tactics for these patients, the type of surgical intervention: conservative, surgical (partial resection, complete resection of the jaws), palliative, pre- and post-medication preparation of the body for intervention.
Relevance
In recent years, the number of cases of medication-associated osteonecrosis of the jaws has increased in dentistry. This is associated with the use of anti-osteoclastic drugs, such as bisphosphonates, monoclonal antibodies (denosumab), and recombinant hybrid proteins (Aflibercept). It is known that the occurrence of medication-associated osteonecrosis leads to a number of pathological changes. These changes also affect the levels of biomarkers that reflect the nature of bone tissue metabolism and regeneration. They are important in the diagnosis and treatment planning for patients, especially during surgical interventions, due to the risk of osteonecrosis.
Goals and Objectives
Based on the available literature, identify biomarkers of bone remodeling and endothelial dysfunction that have the greatest significance for optimizing the early diagnosis of microcirculation disorders in patients with maxillofacial pathologies.
Materials and Methods
A review of methods for analyzing normal bone regeneration with an assessment of bone tissue biomarkers and regulatory factors. Study of diagnostic regimes and identification of the most valuable and rapid disturbances in bone and endothelial vessels.
The mechanisms regulating the relationship between osteoclasts and osteoblasts are crucial for the biology of bone cells. It has been shown that osteoblasts and osteoclasts can interact with each other through direct cell-to-cell contact, cytokines, and extracellular matrix interactions. Osteoblasts can influence the formation, differentiation, or apoptosis of osteoclasts through several pathways, such as the OPG / RANKL / RANK pathways, RANKL / LGR4 / RANK, Ephrin2 / ephB4, and Fas / FasL. Additionally, cytokines released from resorbed bone matrix, such as TGF-β and IGF-1, also affect osteoblast activity. Regulation of osteoclast action occurs through the following factors: the protein related to parathyroid hormone PTHrP, 1,25-dihydroxyvitamin D3, thyroxine, which increase the number and activity of osteoclasts. The hormone calcitonin and estrogens inhibit osteoclast activity (inhibit RANKL activity, enhance OPG production). Calcitropic hormones and cytokines (such as vitamin D3, parathyroid hormone, prostaglandin E2, IL-11) stimulate osteoclastogenesis. Bacterial LPS and some anti-inflammatory cytokines (TNF-alpha, IL-1,3,6, macrophage and osteoblast prostaglandins) enhance osteoclastogenesis.
Osteocytes make up 95% of the total number of cell types in mature bone tissue. They are formed from osteoblasts after they become surrounded on all sides by mineralized bone matrix. Osteocytes regulate the balance of Ca and P in the body, control the activity of osteoblasts and osteoclasts, and produce small amounts of matrix components and signaling molecules (prostaglandin E2, osteoprotegerin OPG, nitric oxide NO, RANKL, sclerostin, etc.). The intercellular substance of bone tissue (matrix) consists of minerals (hydroxyapatites), proteins (proteoglycans, glycoproteins, lipids, acids, type I collagen in mature tissue and III, IV, V, XI, XIII in regeneration areas).
Research Results and Discussion
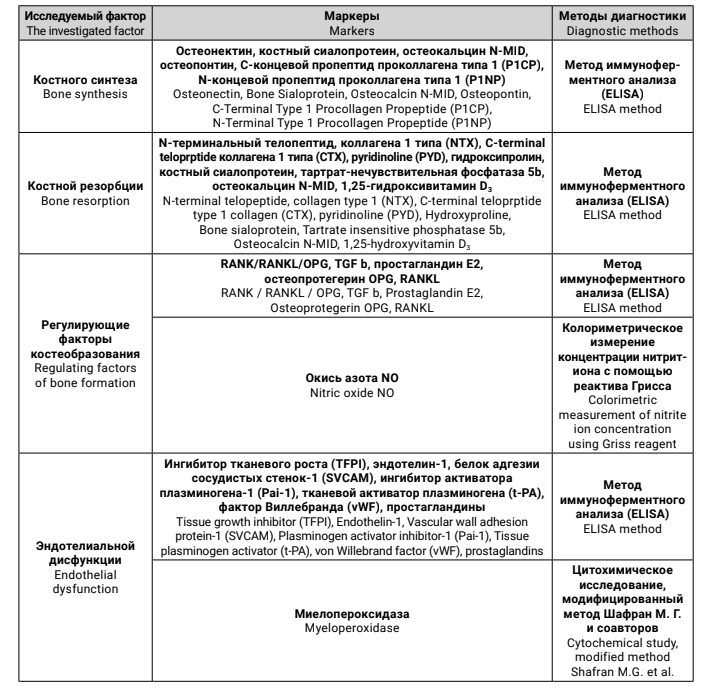
Bone tissue destruction consists of two mechanisms: loss of bone tissue and insufficient replenishment. Bone destruction occurs with the formation of erosive (resorptive) Howship's lacunae. Bone resorption includes: attachment to the bone surface at the resorption site; dissolution of the mineral component of the bone matrix due to acidification of the resorption lacuna to pH 4.5; destruction of organic components by lysosomal enzymes; removal of degradation products from the lacuna by their leakage into the light zones (“decompression” of the zone of tight attachment of the osteoclast to the bone matrix). In bone, loss of the protein matrix and increased bone resorption lead to osteoporosis and can result in pathological fractures and decreased trabecular growth. Increased RANKL likely causes osteoclast-induced bone resorption and bone destruction and may help explain why patients with osteomyelitis experience significant bone mass loss. In 2003, the first reports describing osteonecrosis of the jaw in patients receiving bisphosphonates were published. In the latest protocol from 2014, AAOMS changed the term to medication-related osteonecrosis of the jaw (MRONJ). Recently, there has been a sufficient number of studies indicating the most significant biomarkers of bone regeneration for clinicians (Table 1).
TRAP is expressed by osteoclasts during bone resorption, and TRAP activity in serum correlates with resorptive activity in bone metabolism disorders. TRAP 5b is used as a benchmark for the activity and quantity of osteoclasts and can be specifically detected in serum using immunological assays.
In the study of bisphosphonate-induced osteonecrosis, TRAP staining showed that the number of TRAP-positive (activated) osteoclasts decreased with ZOL treatment (number of TRAP-positive cells: control group, 5.5 ± 1.4; ZOL group, 3.0 ± 2.1). There were no significant differences between the groups. Prior to immunohistochemistry, endogenous peroxidase activity was inhibited by sections incubated in hydrogen peroxide. The sections were subjected to antigen retrieval with citrate-phosphate buffer (pH 6.0). To assess the cellular response during bone remodeling, primary antibodies against OPG, RANKL, and TRAP were used, polyclonal antibodies produced in goats (Santa Cruz Biotechnology, Dallas, Texas, USA). TRAP 5b can be specifically detected in serum using immunohistochemical analysis (IHC) as early as the seventh day after the first administration of denosumab to rats. This indicates that denosumab suppresses the formation of mature osteoclasts in vivo. Since denosumab causes osteonecrosis without a cytotoxic effect per se, it can be assumed that necrosis occurs due to structural changes, such as non-resorbable bone surfaces or lack of vascular ingrowth. The histochemical assessment methodology is described in the experimental model of jaw osteonecrosis in rats on denosumab treatment by Williams et al (2014) – the maxilla and femur were isolated from rats, fixed in 4% paraformaldehyde, with a buffer solution at pH 7.4, at 4 degrees for one day, and then fixed in 70% ethanol. Subsequently, micro-computed tomography scanning was performed, after which the obtained tissues were decalcified in 5% EDTA and 4% sucrose in buffer pH 7.4.
Bone-specific alkaline phosphatase (BALP) is produced from bone into the serum in adults with normal liver function. For the immunoassay of BALP, the detection limit is 0.7 U/L, and the average values are 24.9 ± 7.0 U/L and 19.7 ± 5.6 U/L for men and premenopausal women, respectively. Thus, BALP may be a marker of choice for the early diagnosis of bone metabolism disorders.
Serum osteocalcin is considered a specific biomarker of osteoblast function for assessing the rate of bone tissue formation in osteoporosis. An increase in intact osteocalcin in the serum reflects the synthesis of new osteoblasts. After entering the bloodstream from the extracellular fluid, osteocalcin undergoes rapid proteolytic degradation into polypeptide fragments: amino acids 1–19 (N-terminal), 20–43 (MID), 1–43 (N-MID), 44–49 (C-terminal), 20–49 (MID-C).
The cross-linked carboxy-terminal telopeptide of type 1 collagen (CTX-1, C-terminal telopeptide, CrossLaps) is a product of type 1 collagen degradation. α- (young age) and β-isomers (adults) of CrossLaps are distinguished. In bone metastasis, there is more than a 20-fold increase in the concentration of CrossLaps in the serum, its level increases after menopause and returns to normal one year after bisphosphonate therapy. In situations with increased bone remodeling, type I collagen is broken down by osteoclasts, which release CrossLaps molecules. The study by Marx RE et al found that the risk of complications after surgical interventions in the oral cavity, including the development of osteonecrosis, correlates with the amount of CrossLaps in the serum.
Receptor activator of nuclear factor kappa-B ligand (RANKL) in human serum, according to studies, indicates the presence of metabolic bone diseases. There are several studies that indicate biochemical markers in the diagnosis of thrombosis and endothelial dysfunction. vWF plays a central role in primary hemostasis, where it mediates the adhesion of platelets to the damaged vascular subendothelium and then platelet aggregation. Experimental data indicate von Willebrand factor as an inhibitor of angiogenesis dependent on vascular endothelial growth factor (VEGF), exerting its action through intracellular and extracellular mechanisms involving avb3 and angiopoietin-2, which serve as ligands for von Willebrand factor. Tissue factor pathway inhibitor (TFPI) may influence angiogenesis independently of TF through sequences in its carboxyl terminus (C-TFPI), blocking the activation of VEGF receptor 2 and weakening the migratory capacity of endothelial cells. Elevated levels of TFPI in plasma during inflammatory conditions may lead to endothelial dysfunction. Syndecan-1 is a heparan sulfate proteoglycan of the cell surface that regulates the inflammatory response, proliferation of smooth muscle cells (SMC) during vascular injury, and is prognostically necessary for determining the dynamics of the inflammatory response in the body.
Conclusion
The baseline level of these markers allows for the assessment of the overall state of metabolic processes in bone tissue, as well as justifying the possibility of discontinuing medications that have caused necrotic changes in the jaws. It is known that medication-associated jaw necrosis occurs against the background of taking medications (aminobisphosphonates, monoclonal antibodies, narcotic phosphate-containing substances) after trauma, such as tooth extraction. For example, performing the aforementioned markers in patients with medication-related osteonecrosis of the mandible at long-term follow-up (six months or more) is necessary for monitoring resorption. In osteoporosis, the activity of bone-specific alkaline phosphatase was found to be 66.4 ± 8.7 U/L in women over 59 years old. The average level of osteocalcin showed a significant difference between postmenopausal osteoporosis (16.16 ± 4.50 ng/ml) and non-osteoporotic (11.26 ± 3.07 ng/ml) women. The absence of von Willebrand factor in serum indicates pronounced angiogenic processes: in vitro models have demonstrated a significant increase in endothelial cell proliferation in the absence of von Willebrand factor. Patients with osteonecrosis exhibit a decrease in VEGF. The study of bone tissue degeneration markers and vascular markers allows for a clearer understanding of the principles of osteonecrosis development and, consequently, a more precise prediction, identification of potential markers of inflammatory response and bone degeneration, as well as the appropriate selection of treatment tactics for these patients, the type of surgical intervention: conservative, surgical (partial resection, complete resection of the jaws), palliative, pre- and post-medication preparation of the body for intervention.
G.A. Kosach, S.I. Kutukova, T.D. Vlasov, A.I. Yaremenko
References
Marx RE, et al. Oral bisphosphonate-induced osteonecrosis: risk factors, prediction of risk using serum CTX testing, prevention, and treatment. Journal of oral and maxillofacial surgery: official journal of the American Association of Oral and Maxillofacial Surgeons. 2007. 65(12):2397-410 doi: 10.1016/j.joms.2007.08.003
Sales Lima MV1 de, et al. Denosumab Related Osteonecrosis of Jaw: a Case Report. Journal of Oral and Maxillofacial Research. 2018;Dec;30;9(4):e5. doi: 10.5037/jomr.2018.9405
Mawardi H, et al. Osteonecrosis of the jaw associated with ziv-aflibercept. Journal of Gastrointestinal Oncology. 2016 Dec;7(6):E81-E87. doi: 10.21037/jgo.2016.05.07
Harold N Rosen. Use of biochemical markers of bone turnover in osteoporosis. Clinical Chemistry and Laboratory Medicine. 2008;46(10):1345-57. doi: 10.1515/CCLM.2008.310
Del Fattore, Andrea, Anna Teti, and Nadia Rucci. Osteoclast receptors and signaling. Archives of biochemistry and biophysics. 2008;473(2):147-60. doi: 10.1016/j.abb.2008.01.011
Chen X, et al. Osteoblast–osteoclast interactions. Connective tissue research. 2018;59(2):99-107. doi: 10.1080/03008207.2017.1290085
Kathryn L, ed. Pathophysiology: The Biologic Basis for Disease in Adults and Children. 8 edition. 2019. Available from: https://vk.com/doc313186384_520259268?hash=08f64 af1b82bfc6a95&dl=c27e5d0e4f93077aa1
Brad W.Neville, et al. Periodontal Pathology, in Color Atlas of Oral and Maxillofacial Diseases. 2019;93-107. https://doi.org/10.1016/B978-0-323-55225-7.00004-X
Marx RE. Pamidronate (Aredia) and zoledronate (Zometa) induced avascular necrosis of the jaws: a growing epidemic. Journal of oral and maxillofacial surgery: official journal of the American Association of Oral and Maxillofacial Surgeons. 2003;61(9):1115-7. doi: 10.1016/S0278-2391(03)00720-1
Ruggiero SL et al. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw-2014 update. Journal of oral and maxillofacial surgery: official journal of the American Association of Oral and Maxillofacial Surgeons. 2014;Oct;72(10):1938-56. doi: 10.1016/j.joms.2014.08.017