
Experimental Study of Fractional Laser Impact on the Schizoid Membrane in the Dental Implantation Area
Machine translation
Original article is written in RU language (link to read it) .
Lasers have long been used in dentistry, but the search for new concepts continues to this day. The fractional laser technology is a new treatment method using a diode laser that was proposed at the beginning of this century. Laser Patterned Microcoagulation (LPM) can be explained by the formation of damaged areas (ablation) in the tissue surrounded by viable tissue. The process of tissue regeneration can be regulated and optimized by properly selecting laser parameters such as wavelength, pulse duration, and the size of microcoagulation columns.
The issue of soft tissue volume in the area of dental implantation has recently received much attention in both domestic and foreign literature.
Na T.J., Tinti C. showed that the volume of attached keratinized gingiva can disappear after implant placement. Wennstrom J. L. in his article demonstrated that even a minimal volume of attached keratinized gingiva positively affects the long-term stability of soft tissues.
A number of authors associate the survival of implants in the lateral section of the mandible with the presence of keratinized gingiva and the patient's ability to maintain individual hygiene of the restoration.
Thus, the long-term stability of implants is influenced by the volume of bone tissue, the amount of attached keratinized gingiva, individual oral hygiene, and the correct positioning of restorations supported by implants. And although a direct link between the absence of attached keratinized gingiva and the long-term survival of the implant has not been proven, clinical practice clearly welcomes the presence of this gingiva around its superstructures.
Therefore, a lack of keratinized gingiva can be considered one of the factors that leads to mucositis, and subsequently to peri-implantitis and disintegration of the dental implant.
Figure 1 shows a clinical case: eight years ago, implants were placed in the patient, however, he ignored professional oral hygiene.

In Figure 2, there is an implant in the third sector with improper positioning and a distal cantilever, which has led to the development of peri-implantitis.

The volume of keratinized gingiva is traditionally restored surgically. The main methods for recreating the volume of attached gingiva fall within the realm of surgical periodontology and are represented by several procedures. The primary procedure used by surgeons is the connective tissue grafting. Free gingival grafts, allografts, flap displacement, and others are also used. In certain indications, vestibuloplasty is performed to recreate the area of attached but non-keratinized gingiva, with the aim of improving care for restorations. These techniques are quite traumatic and require appropriate surgical skills.
In clinical periodontology, the concept of LPM (laser pattern microcoagulation) is already effectively used for the prevention of recessions and control of periodontal infection.
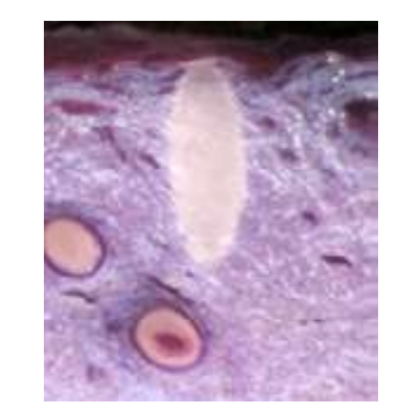
In Figure 3, you can see the use of lasers in periodontology and the histological picture of microcoagulation columns (Fig. 4), which remain in the gingiva after the procedure.

Purpose of the Study
To study the effect of fractional laser on the mucous membrane of the oral cavity in the area of dental implantation to increase the volume of attached keratinized gingiva or to enlarge the area of attached mucosa.
Materials and Methods of the Study
The study involved:
patients with previously installed Nobel Biocare Replace Conical Connection implants, ranging from two to four implants using a two-stage technique;
patients with an uncomplicated postoperative period;
a time period of one to three months after implant installation;
during the visual examination of these patients and determining the mucogingival junction using the roll technique, an insufficient area of attached keratinized gingiva was identified;
the diameter of the attached gingiva was 2 mm or less. These patients were offered to undergo a course of laser therapy instead of a rather complex surgical intervention for gingival plastic surgery in the implant area. 21 out of 30 individuals agreed to this procedure even without a guarantee of success.
The study did not include:
patients with scarred mucosa, presence of vestibular bands in the implantation area;
patients who were set for surgical treatment due to time constraints;
patients with previously installed gingival cuff formers.
The exposure was conducted using the Alta ST laser device. We used a mode with a pulse duration of 100 to 170 ms, an output power of 25 W, and a working tip diameter of 320 μm. Single exposures were performed in the amount of 30-40 pieces.
Under topical anesthesia, laser applications were performed along the mucogingival junction and then spreading to the unattached mucosa, with the aim of covering 15% to 30% of the surface area of the exposure zone. The exposure itself was conducted perpendicular to the surface of the mucous membrane. The procedure was performed once every two weeks for a total of four sessions. During each exposure and two weeks after the last one, photography was conducted using a template with a diameter of 3 mm. To more accurately determine the boundary of the transition from attached mucosa to unattached, a standard roll method was used. Additionally, during each session, a survey was conducted to assess the degree of pain from this exposure, and we recorded changes in the transition from movable mucosa to immovable.
Clinical Case 1
A 52-year-old female patient underwent augmentation of the alveolar ridge of the lower jaw on the left side with bone blocks. Three dental implants were then placed. One month after placement and with an uncomplicated postoperative course, an insufficient area of attached keratinized gingiva was noted, especially in the area of the missing first premolar. The treatment was conducted according to the proposed scheme (fig. 5—8).




Clinical Case 2
A 50-year-old female patient had three implants placed in the upper jaw. In the area of the middle implant, there was an insufficient zone of attached keratinized gingiva. After four sessions of laser treatment according to the scheme, we observed a reduction in the mobility of the vestibular tissues, which allowed us to place the gingival cuff formers without a plastic surgery on the soft tissues in the implantation area (fig. 9-11).



Clinical Case 3
A 55-year-old patient had two implants placed in the upper jaw. A bridge prosthesis was planned to be made supported by the two implants. The patient was offered to undergo four sessions of laser treatment to avoid an additional surgery for increasing the volume of soft tissues in the area of the implants (Fig. 12-14).



Conclusions
Fractional laser microcoagulation is a practically painless method of affecting the mucous membrane of the oral cavity.
There are no complications when laser exposure is applied to the mucous membrane of the oral cavity.
In 7 out of 11 cases, a visually detectable increase in the area of keratinization of the gums or attachment of the movable mucosa to the alveolar process occurred.
In 64% of cases, the installation of gingival cuff formers on implants after laser exposure was performed without additional surgical intervention.
The results obtained provide a basis for further study of the effect of laser radiation on the regeneration of the mucous membrane of the oral cavity and, in particular, keratinized gums.
A.I. Yaremenko, A.Yu. Zernitsky, E.A. Zernitskaya
List of References
Gladkova N. D., Karabut M. M., Kiseleva E. B., Ostrovskaja Yu. V., Muraev A. A., Balalaeva I. V., Fel'dshtejn F. I. In vivo control of the regeneration of the oral mucosa after fractional laser photothermolysis using cross-polarization optical coherence tomography // Modern Technol. Med. 2012. No2. P. 13-19.
Gladkova N, D., Karabut M, M., Kiseleva E, B., Ostrovskaja Yu, V., Muraev A. A., Balalaeva I. V., Fel'dshtejn F. I. In vivo control of the regeneration of the oral mucosa after fractional laser photothermolysis using cross-polarization optical coherence tomography // Modern Technol. Med. 2012, No2. P. 13-19.
Karakov K. G., Hachaturjan E. E., Seiranidu Z. A. Clinical experience of using a laser photodynamic system in dentistry // Periodontology, 2012. No1 (62), P. 61-63.
Karakov K, G., Hachaturjan E. E., Seiranidu Z. A. Clinical experience of using a laser photodynamic system in dentistry // Periodontology. 2012, No 1 (62), P. 61-63.
Yaremenko A. I., Zernickij A. Yu., Zernickaja E. A. Experimental study of fractional laser impact on bone tissue regeneration in the augmentation zone // Periodontology. 2016. No 1 (78). P. 18-21.
Yaremenko A. I., Zernickij A. Yu., Zernickaja E. A. Experimental study of fractional laser impact on bone tissue regeneration in the augmentation zone // Periodontology. 2016. No1 (78). P. 18-21.
Block M. S., Gardiner D., Kent J. N., Misiek D. J., Finger I. M., Guerra L. Hydroxyapatite-coated cylindrical implants in the posterior mandible: 10-year observations // International Journal of Oral & Maxillofacial Implants, 1996, Vol. 11. Issue 5, P. 15.
Han T. J., Klokkevold P. R., Takei H. H. Strip gingival autograft used to correct mucogingival problems around implants // Int J Periodontics Restorative Dent. 1995, Aug. No15 (4), P. 404-411.
Lang N, P., Nyman S, R, Supportive maintenance care for patients with implants and advanced restorative therapy // Periodontol 2000, 1994, Feb. No4, P. 119-126.
Romanos G. E., Gladkova N. D., Feldchtein F. I., Karabut M. M., Kiseleva E, V., Snopova L, B, et al. Oral mucosa response to laser patterned microcoagulation (LPM) treatment. An animal study // Lasers Med Sci. 2013. Jan. No28 (1), P. 25-31.
Roos-Jansåker A. M., Renvert H., Lindahl C., Renvert S. Nine- to fourteen-year follow-up of implant treatment, Part III: factors associated with peri-implant lesions // J Clin Periodontol. 2006. Apr. No33 (4), P. 296-301.
Tinti C., Parma-Benfenati S, Coronally positioned palatal sliding flap // Int J Periodontics Restorative Dent. 1995. Jun. No 15 (3), P. 298-310.
Wennström J, L, Lack of association between width of attached gingiva and development of soft tissue recession. A 5-year longitudinal study // J Clin Periodontol. 1987, Mar, No 14 (3), P. 181-184.