
Airway Dentistry Guide: OSA Diagnostics & Evidence-Based Treatment
Airway dentistry represents an interdisciplinary interface between sleep medicine, craniofacial development, and clinical dental practice. In recent years, the field has expanded beyond traditional oral appliance therapy to include a range of structural, functional, and behavioral interventions targeting obstructive sleep apnea (OSA) and related sleep-disordered breathing (SDB).
However, the rapid growth of these approaches has outpaced the strength of supporting evidence in several domains. While certain therapies, most notably oral appliance therapy, are supported by robust clinical data, many emerging interventions remain adjunctive, technique-sensitive, or insufficiently validated as standalone treatments.
This article aims to present a structured, evidence-informed framework that distinguishes established therapies from evolving concepts, while clarifying the dentist’s role within an interdisciplinary model of care.
The Anatomy of Obstruction. From Pathophysiology of Airway Dysfunction to Life-Saving Intervention
To effectively communicate with both patients and medical colleagues, dental professionals must understand that Obstructive Sleep Apnea (OSA) is not a localized airway issue but a systemic inflammatory disease. While Sleep-Related Breathing Disorders (SRBD) encompass a spectrum, including snoring.
The Biological Necessity of Nasal Breathing
As dentists, we often see the "end-stage" results of airway dysfunction: worn teeth, crowded arches, and inflamed gums. However, the background cause is frequently a breakdown in the most basic human function: nasal breathing. The nose is not merely a passage; it is a sophisticated climate-control and filtration system.
- The Nitric Oxide Factor: Nasal breathing adds small amounts of nitric oxide (NO) to the air. NO is a potent vasodilator and antimicrobial agent that reduces lung inflammation.
- Filtering and Warming: The nose filters pathogens and regulates the temperature and moisture of inspired air, benefits that mouth breathing completely bypasses.
- Craniofacial Growth: Proper nasal breathing allows the tongue to rest against the anterior roof of the mouth, acting as a natural scaffold for a wide, U-shaped maxilla and mandible.
Pathophysiology: The Cycle of Obstruction
An obstructive apnea is defined as a cessation of breathing (90% reduction in airflow) lasting at least 10 seconds, despite continued respiratory effort. These events typically last 10–30 seconds but can exceed a minute.
- The Mechanical Trigger: During Rapid Eye Movement (REM) sleep, the dilator muscles of the upper airway (geniohyoid, genioglossus, tensor veli palatini) lose their tone. In patients with anatomical predispositions (large tongue, retrognathia, or obesity), this leads to airway collapse.
- The Physics: The negative pressure of inspiration acts like a vacuum, drawing the base of the tongue and the soft palate posteriorly against the pharyngeal walls.
- The Physiological Cost: The resulting asphyxia (hypoxaemia and hypercarbia) terminates with a "micro-arousal" – a cortical "jolt" that restores muscle tone to open the airway. In severe cases, this cycle repeats hundreds of times per night, leading to profound sleep fragmentation and systemic oxidative stress.
Comorbidities: The "Silent Killer" Connections
Untreated OSA is strongly associated with several life-threatening conditions. When educating patients, dentists should highlight these evidence-based links:
- Hypertension: Present in nearly 50% of all OSA cases.
- Cardiovascular Disease: Significant correlation with atrial fibrillation, acute coronary syndrome, and fatal cardiac events.
- Metabolic Health: Direct link to Type 2 Diabetes and obesity.
- Neurological Impact: Increased risk of stroke, transient ischemic attacks, cognitive impairment, and a higher incidence of dementia.
- Mental & Sexual Health: Strong associations with depression, mood disorders, and sexual dysfunction.
The Dentist’s Diagnostic Checklist
A dentist is often the first healthcare provider to identify "occult" (hidden) OSA. During a comprehensive exam, look for these Salient Markers:
- Physical Anatomy: A neck circumference >42.5 cm, a Body Mass Index (BMI) >29 kg/m², and macroglossia (enlarged tongue).
- Radiographic Clues: On panoramic or lateral cephalometric films, look for calcified carotid artery atheromas. These are present in roughly 20% of OSA patients and are a direct marker of stroke risk.
- Jaw Position: Micrognathia (small jaw) or retrognathia (receded jaw) which reduces the "functional space" for the tongue, forcing it toward the pharynx.
The Treatment Landscape: PAP vs. OAT vs. Surgery
While the dental office is the primary site for Oral Appliance Therapy (OAT), we must understand the broader therapeutic context to better advise our patients:
- Behavioral Modification: Weight loss, exercise, and avoiding alcohol (which increases OSA risk by 25%) are critical first steps.
- Positional Therapy: Up to 50% of cases are classified as "supine-related." For these patients, side-sleeping can significantly reduce AHI levels.
- Positive Airway Pressure (PAP): The medical "gold standard." However, due to mask discomfort and dryness, compliance rates are low, ranging from 17% to 60%.
- OAT (Mandibular Advancement): Custom-made, titratable devices are the preferred alternative for those who cannot tolerate PAP. They are simpler, have higher patient preference, and better long-term compliance.
- Surgical Interventions: Options like Uvulopalatopharyngoplasty (UPPP), Maxillary-Mandibular Advancement (MMA), or Hypoglossal Nerve Stimulation (an implantable device that moves the tongue forward) are reserved for cases where non-surgical options fail.
Clinical Summary for the Dental Team
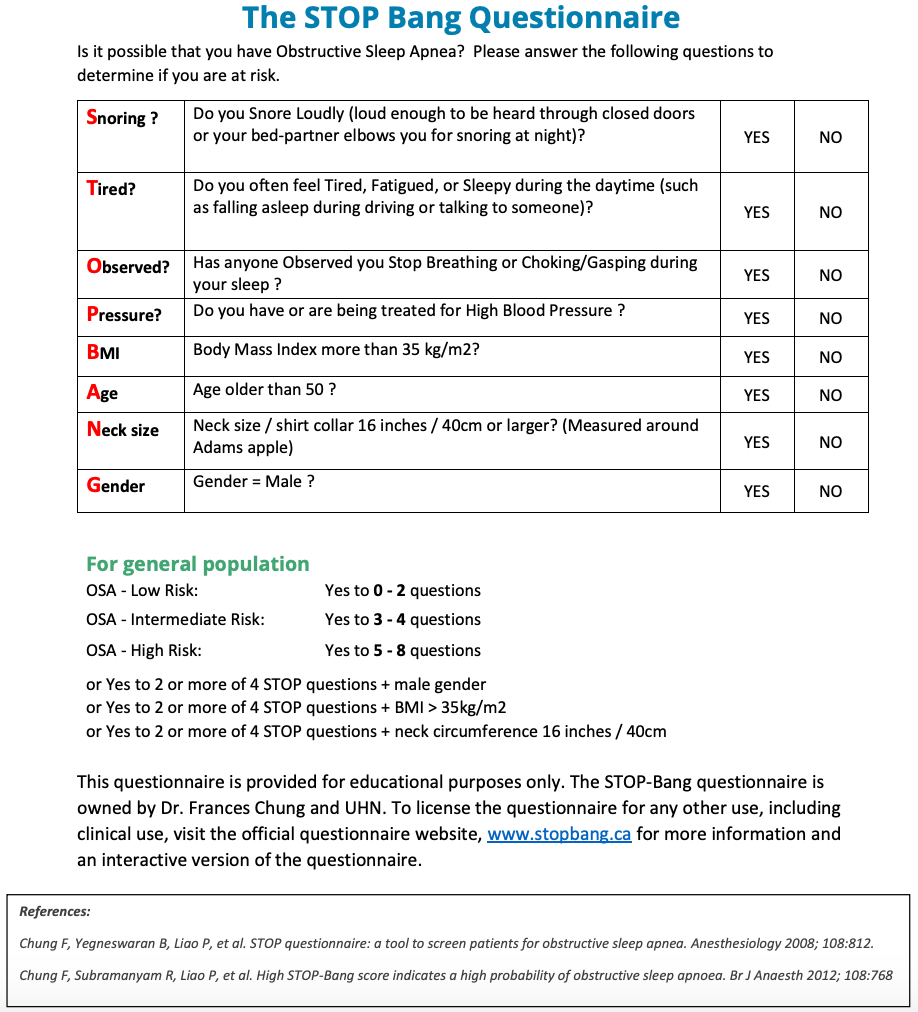
The goal of integrating this data into your practice is to reduce OSA-related morbidity and mortality. By screening for a high-arched palate, macroglossia, and a large neck circumference, and by using validated tools like the Berlin Questionnaire or STOP-Bang, you are performing life-saving preventative medicine.
Remember: A patient who complains of "dry mouth on awakening" or "morning headaches" isn't just a candidate for a night guard, they are likely a candidate for a life-changing airway evaluation.
The Dentist’s Role and The Collaborative Clinical Pathway
Effective management of Obstructive Sleep Apnea (OSA) is inherently interdisciplinary.
- Two Pathways to Care: Patients typically enter treatment either through dental screening (followed by medical referral for diagnosis) or via direct referral from a physician for OAT.
- The Physician's Role: Regardless of who initiates the screening, the final diagnosis of OSA must be made by a medical provider.
- The "Qualified Dentist" (QD): To provide high-standard care, dentists should ideally hold diplomate certification or have completed standardized evidence-based training (like the AADSM Mastery Program).
Screening and Comprehensive Assessment
A thorough evaluation is the foundation of successful therapy. Screening should not be limited to "known" sleep patients but integrated into general dental check-ups.
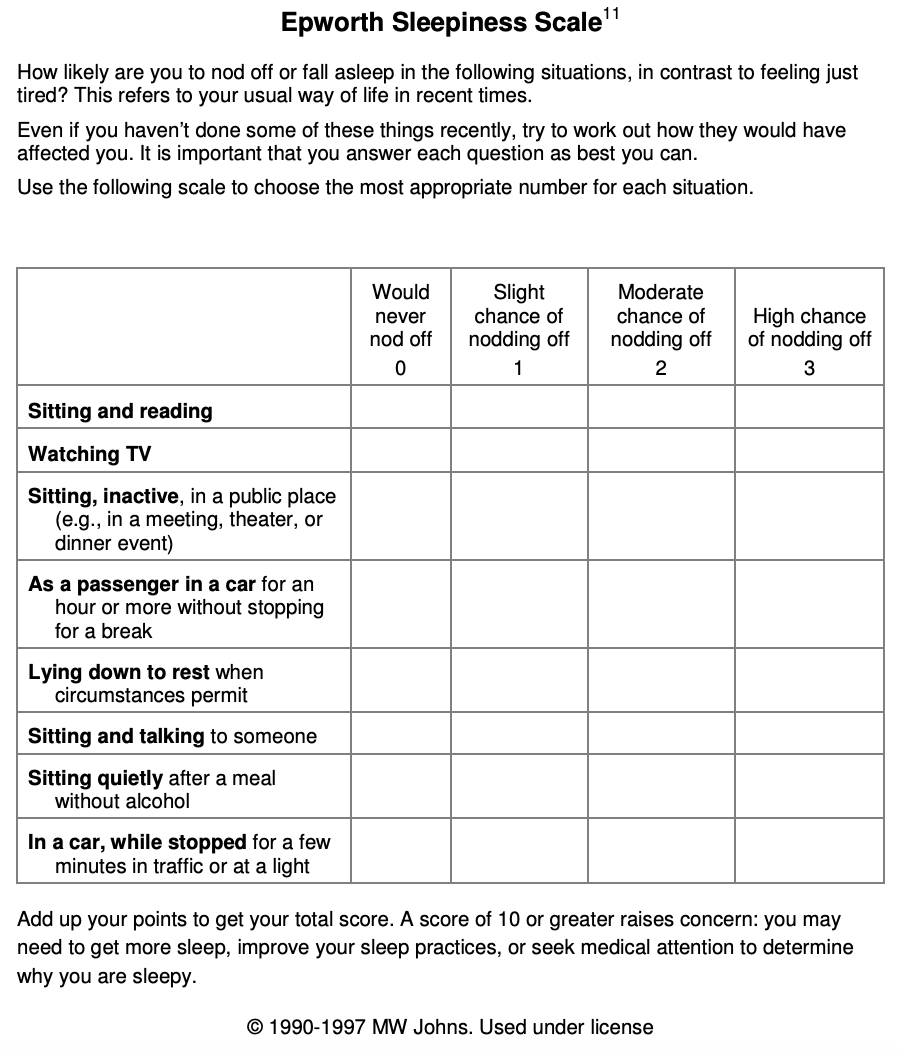
- Validated Tools: Utilize instruments like the STOP-BANG Questionnaire and the Epworth Sleepiness Scale (ESS) to assess risk and subjective sleepiness.
- Clinical Indicators: Look for physical markers during the oral exam, including posterior pharyngeal crowding, macroglossia, signs of sleep bruxism, and enamel erosion (often linked to GERD).
- Diagnostic Referral: If OSA is suspected, collaborate with a physician for the diagnostic interpretation.
Take your role as a leading specialist in the fight against sleep apnea by mastering the functional physiology of respiratory impairment. Join world-renowned expert Professor Roger Price in the course “Airways for Dentist” to integrate functional diagnostics and integrative medicine into your airway treatment protocols.
The basic problem of airway dysfunction is structural. If we can improve a child's airway development early, we can prevent the systemic comorbidities of adulthood.
The Multi-Disciplinary Referral Network: A standard of care now requires every patient to receive an airway questionnaire and physical exam. When dysfunction is suspected, your referral "dream team" should include:
- Airway-Centric Orthodontist (for skeletal expansion).
- ENT (to clear nasal obstructions/tonsils).
- Myofunctional Therapist (to retrain tongue posture and nasal breathing).
- Sleep MD (for definitive diagnosis).
By focusing on education and early intervention, we move from treating symptoms to ensuring our patients live longer, healthier lives.
Diagnostic Framework. Imaging Modalities and the Postural Variable
In the quest to normalize the maxillofacial system and airways, the quality of our data dictates the success of our treatment plan. While traditional 2D imaging remains a staple in orthodontics, emerging research highlights significant limitations and potential solutions in how we visualize the "collapsible tube" of the human airway.
1. Navigating the Three Compartments
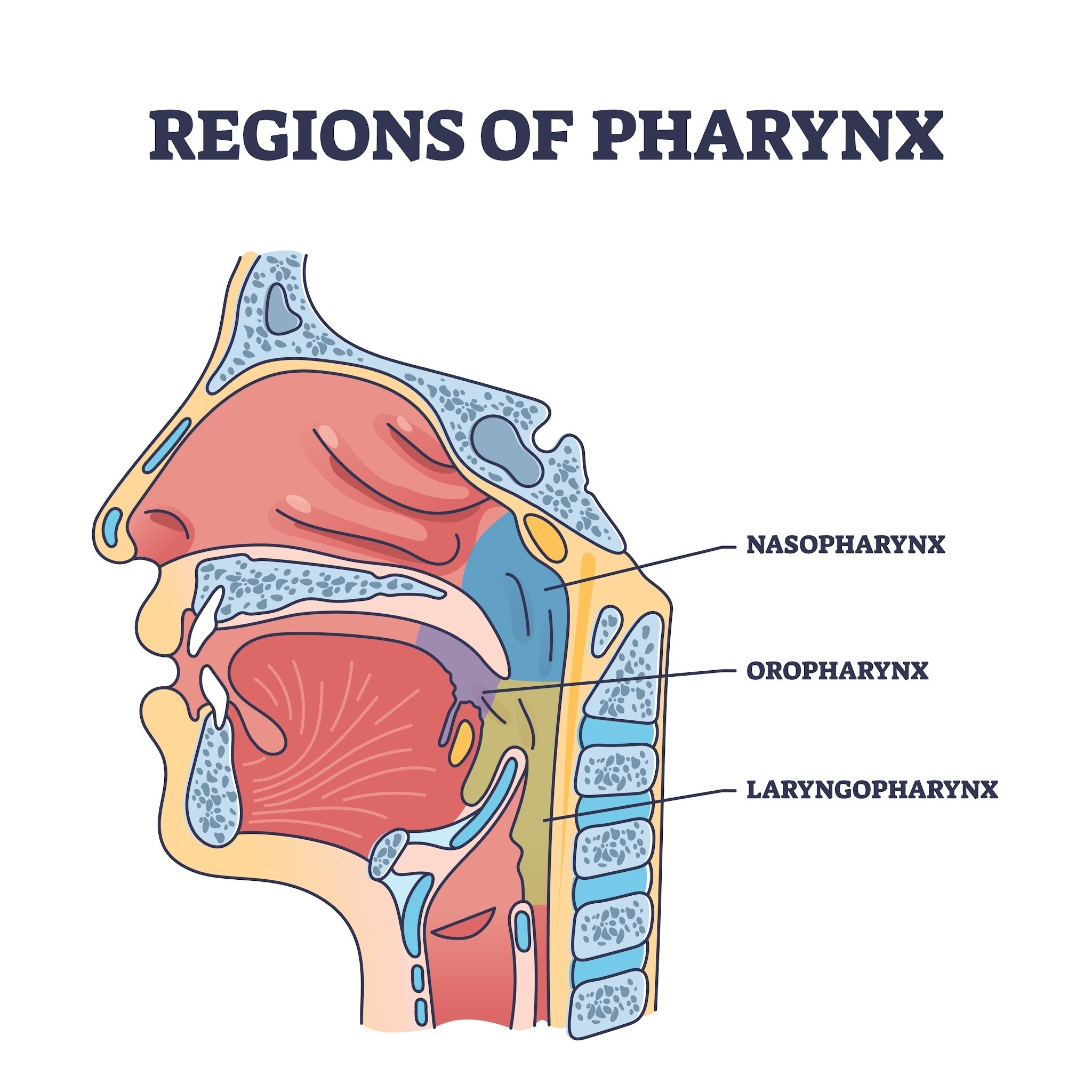
For diagnostic purposes, the upper airway is divided into three distinct anatomical regions. Understanding their structure explains why some areas collapse while others remain stable:
- Nasopharynx: The most stable region because it is surrounded by rigid bony structures.
- Oropharynx: The most susceptible to collapse. It is surrounded entirely by soft tissue and is highly influenced by external factors like posture and muscle tone.
- Hypopharynx: Located lower in the airway, this region is generally less sensitive to postural changes in healthy (non-OSA) individuals, but its size is significantly reduced in OSA patients when supine.
2. The "Postural Trap": Standing vs. Supine
A major challenge in airway dentistry is that most dental imaging (like Cephalometry or CBCT) is performed while the patient is standing or sitting, yet the pathology we are treating (OSA) occurs while the patient is supine (lying down).
- Gravitational Effects: When a patient moves from a standing to a supine position, gravity and upper airway reflexes cause the tongue and soft palate to shift backward, increasing the thickness of the soft tissues and narrowing the oropharyngeal space.
- Imaging Discrepancy: Research shows that standing cephalometric scans often yield larger airway measurements than supine MRI scans. Relying solely on standing measurements may lead a clinician to overestimate the airway’s patency during sleep.
3. Evaluating Our Diagnostic Toolkit
How do our common imaging tools stack up against the "Gold Standard" of 3D volumetric data?
| Modality | Dimension | Posture | Advantages | Limitations |
| Cephalometry | 2D | Standing | Widely available, low cost, long clinical history. | 2D linear measurements only; superimposition of bilateral structures; poor volume prediction. |
| Kinetic MRI | 2D Dynamic | Supine | No radiation; shows dynamic changes/function; mimics sleeping posture. | Limited availability in standard dental settings. |
| 3D MRI / CBCT | 3D Volumetric | Supine/Standing | Provides total volume and "MinAx" (minimal axial area). | MRI is the "gold standard" for soft tissue; CBCT is superior for bone but involves radiation. |
4. Predictive Value: What Actually Matters?
The goal of imaging is to predict the airway volume and the likelihood of collapse. Recent studies have found:
- Kinetic MRI is a stronger predictor: Because kinetic MRI is taken in a supine position (consistent with sleep), it has a significantly higher correlation (Spearman’s rho > 0.60) with actual 3D airway volume than standing cephalometry.
- The Retropalatal Area (RPA) is Key: Both 2D and 3D imaging suggest that the retropalatal region is one of the most critical predictors of airway narrowing and OSA severity.
- The Hypopharyngeal Correlation: Interestingly, the hypopharyngeal area measured on a 2D standing cephalogram does correlate well with 3D volume. This is because this specific region is less affected by posture in non-OSA subjects.
Clinical Implementation: How to Choose?
The selection of your imaging modality should be driven by your specific clinical question:
- For Routine Orthodontic Planning: Cephalometric imaging remains a valuable tool for identifying general airway dimensions and skeletal relationships.
- For High-Risk OSA Patients: If you suspect a high risk of collapse, seek imaging that reflects the supine position. Supine MRI or CBCT provides more "physiological" information that mirrors the patient’s state during sleep.
- For Functional Assessment: Kinetic MRI is superior for observing how the soft tissues move during breathing and swallowing without the burden of radiation.
Professional Takeaway
We must look beyond the static, standing 2D image. By acknowledging that the airway is a dynamic 3D structure, and that its dimensions "shrink" the moment our patients lie down, we can refine our diagnostic protocols and provide more predictable, life-saving outcomes in orthodontic and airway practice.
Evidence-Based Treatment Modalities
1. Skeletal and Dental Malocclusion Interventions
Malocclusion is a significant risk factor for airway issues, often associated with maxillary constriction and mandibular retrusion.
- Functional Appliances: These customized devices advance the mandible in growing children. While they improve dental relationships, it remains unclear how much of this correction is due to the appliance versus natural growth.
- Implementing Oral Appliance Therapy (OAT)
OAT is a proven, first-line therapy for primary snoring and a highly effective alternative to PAP therapy for mild-to-severe OSA.
- Appliance Selection: Evidence supports the use of custom-fabricated, adjustable dual-arch appliances. Selection should be patient-centered, considering manual dexterity, restorative needs, and nasal patency.
- The Construction Bite: Impressions and bite records should be performed in person. While the initial protrusive setting is at the clinician's discretion, a range of 25% to 75% is typically both comfortable and therapeutic.
- Vertical Dimension Caution: While adjusting the vertical dimension is often necessary for fabrication, clinicians should be aware that excessive vertical opening can actually reduce the appliance's efficacy.
- Calibration, Compliance, and Long-Term Success
The "delivery" of the appliance is only the beginning of the treatment journey.
- Titration and Calibration: Evaluate the patient within 30 days of insertion. Advancement should be guided by the resolution of symptoms and, where appropriate, objective data from pulse oximetry or HSAT.
- Defining Compliance: For OAT to be considered successful, patients should aim for "full compliance," defined as wearing the appliance for ≥80% of the night for more than 5 nights per week.
- Ongoing Management: Patients require follow-up every 6 months during the first year, and annually thereafter. These visits are crucial for monitoring occlusal stability, checking the structural integrity of the device, and managing potential side effects like TMJ discomfort or tooth movement.
- Maxillary Expansion (RME): Rapid maxillary expansion aims to lower nasal resistance and improve pharyngeal dynamics.
- Guideline: Expansion should only be considered if a transverse discrepancy is present; it is not currently recommended to treat OSA or snoring in isolation.
- Adult Considerations: Expansion in adults often requires surgical assistance or bone-anchored devices to avoid unstable tooth tipping and root resorption.
2. Myofunctional Approaches
Myofunctional strategies focus on the "soft tissue" aspects of the airway, targeting the tongue and oropharyngeal muscles.
- Myofunctional Therapy (MFT): This involves isometric and isotonic exercises to improve the tone and mobility of the orofacial musculature.
- Current Standing: Evidence is insufficient to support MFT as a primary standalone cure for OSA. However, it may have potential as an adjunctive management therapy due to its low risk.
- Professional Training: MFT should be provided by qualified clinicians, such as speech-language pathologists (SLPs), in an interdisciplinary setting.
- Myofunctional Orthodontics: These typically combine myofunctional exercises with prefabricated (rather than customized) removable appliances. The panel found insufficient evidence to support these for preventing or curing adult OSA.
Bridge the gap between theory and practice by mastering the essential link between muscle function and systemic airway health. Join the expert-led online course “Airway and Sleep-Disordered Breathing: Integrating Myofunctional Protocols” to gain the practical skills needed to implement functional orthopedic solutions and holistic myofunctional care in your practice.
3. Tethered Oral Tissues (TOTs)
There has been a massive 870% increase in surgical procedures for tethered oral tissues (such as "tongue-tie") over the last two decades.
- ANKYLOGLOSSIA AND OSA: While short lingual frenums are sometimes observed in pediatric OSA cases, current evidence does not support the claim that ankyloglossia causes OSA.
- Recommendation: Clinicians are urged to scrutinize the necessity of frenectomy procedures, as they can be associated with serious adverse effects in infants and children.
4. Laser Therapy for Snoring and OSA
Laser treatments aim to tighten the soft palate and adjacent tissues to reduce airway vibrations or collapse.
- Nonablative Laser Therapy (NALT): Unlike ablative lasers, NALT does not cause scarring and has fewer side effects.
- Efficacy: Evidence remains uncertain for NALT as a monotherapy. While it often results in high patient satisfaction for snoring reduction, the effects are temporary and typically require annual retreatments.
5. Debunking the "Extraction" Myth
A long-standing controversy in dentistry is whether extracting teeth for orthodontics increases the risk of OSA by reducing airway space.
- Pediatric Findings: High-quality evidence suggests that childhood extractions are not a risk factor for OSA.
- Adult Findings: Studies show no difference in OSA risk between patients with extracted premolars and those with full dentition. Furthermore, moderate retraction can sometimes increase airway dimensions through mesial molar movement.
Clinical Summary
Based on the AADSM consensus, none of these emerging therapies are currently recommended as first-line monotherapies. Instead, they should be viewed as:
- Rescue or Adjunctive Options: Useful when proven therapies (like oral appliances or CPAP) have failed or require supplementation.
- Case-by-Case Interventions: Dentists must use their clinical expertise to weigh the limited evidence against the patient’s unique anatomy and values.
Closing Summary: Toward an Evidence-Guided, Interdisciplinary Model
The integration of airway assessment into dental practice reflects an important shift from a purely tooth-centered model toward a broader understanding of oral-systemic health. Dentists are uniquely positioned to identify early signs of sleep-disordered breathing through routine clinical examination and patient-reported symptoms, making them a critical entry point into the diagnostic pathway.
At present, the strongest evidence supports a structured approach centered on validated screening tools, appropriate medical referral for definitive diagnosis, and the use of established therapies such as oral appliance treatment in collaboration with sleep physicians. Emerging interventions—particularly those targeting craniofacial development and orofacial function—hold promise but require further high-quality research to define their role within standardized care pathways.
A balanced, evidence-informed approach is essential. This includes recognizing both the potential and the limitations of current airway-focused concepts, avoiding overgeneralization, and prioritizing patient safety and long-term outcomes.
Ultimately, optimal management of OSA depends on interdisciplinary collaboration between dentists, sleep medicine specialists, otolaryngologists, and allied health professionals. By integrating systematic screening, appropriate referral, and individualized treatment planning, dental practitioners can contribute meaningfully to the early detection and management of a condition with significant public health impact.