Immediately loaded tilted implants combined with angulated screw channel zirconia abutments in atrophic maxillary patients: a three-year after loading prospective case series study
Summary
Purpose. To evaluate the 3-year clinical and radiographic outcomes of partially edentulous patients treated with immediately loaded tilted implants, combined with angulated screw channel (ASC) zirconia abutments.
Materials and methods. Any patient requiring an implant-supported fixed dental prosthesis for the rehabilitation of the atrophic posterior maxilla and refusing guided bone reconstruction was considered eligible for this study. Two to three immediately loaded flapless implants, combined with immediately placed ASC abutments were placed for each patient. Six months after implant placement/loading a definitive prosthesis was placed. Outcomes were: prosthesis and implant failures, complications, and peri-implant bone level changes. Outcomes were recorded at implant placement/loading and yearly up to 3-year later.
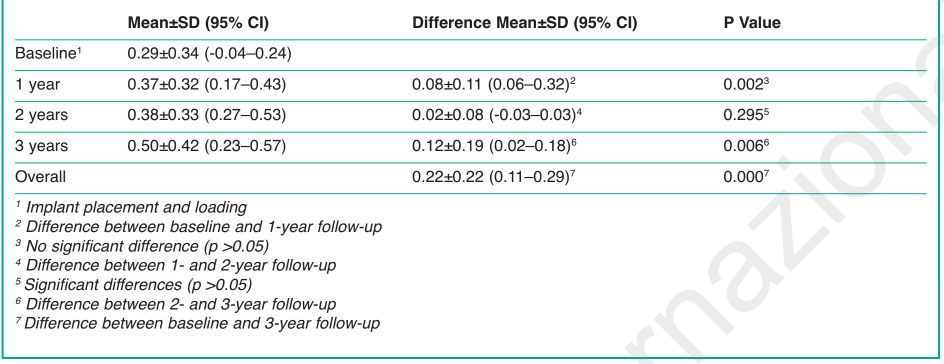
Results. Twenty-three anodized implants and ASC zirconia abutments were placed in 10 consecutive participants (mean age 57.2 years) with severe atrophy of the posterior maxilla, by using computer-guided template-assisted surgery. The mean follow-up period was 38.2 months. No patients dropped out. The prosthesis and implant cumulative survival rate was 100%. No biologic or technical complications were experienced during the entire follow-up. Mean marginal bone levels were 0.29±0.34 mm at implant placement and loading, 0.37±0.32 mm at the 1-year follow-up (difference 0.08±0.11 mm; p=0.002), 0.38±0.33 mm at the 2-year follow-up (difference between the 1- and 2-year follow-up 0.02±0.08 mm; p=0.295), and 0.50±0.42 mm at the 3-year follow-up (difference from implant placement 0.22±0.22 mm; p=0.000).
Conclusions. Guided surgery and immediate loading of ASC zirconia abutment is an effective and reliable treatment option for the treatment of the partially edentulous posterior atrophic maxilla. Further RCT studies are needed to better understand the gold standard approach in such patients.
Introduction
The progressive resorption of the alveolar bone, pneumatization of the maxillary sinus, sinus pathologies, and poor quality of residual alveolar bone, poses significant difficulty for placement of implants in edentulous maxillary jaw without preliminary reconstructive procedures. The remaining bone height is insufficient to support dental implants, and the sinus floor has to be augmented in order to obtain acceptable bone volume for implantation. Such invasive treatment exposes the patient to the risk of increased postsurgical morbidity. Financial costs and healing periods are increased as well.
There are different treatment options for the treatment of posterior atrophic maxilla, such as sinus lift surgery, short implants, distal cantilevers, or zygomatic implants. The clinician also has another possibility to ensure a distal prosthetic support while avoiding grafting procedures, by placing implants tilted distally and mesially parallel to the anterior and posterior sinus wall respectively. The advantages of such implant placement are now well known. First, the possibility of using the entire residual crestal bone enables the placement of longer implants, in order to have an increased bone anchorage and bone-to-implant contact (BIC). Furthermore, it provides a longer inter-implants distance reducing or totally eliminating distal cantilever and resulting in a better implant load distribution. Several prospective studies and systematic reviews concerning the use of tilted implants reported high implant and prosthetic survival rates as well as no adverse effect on bone resorption. However, while the results offered by this treatment are encouraging, it should be highlighted that a high level of surgical skill of the surgeon is crucial, as has been described before in the literature.
A screw-retained restorative connection represent many advantages: minimal interocclusal spaces, highly hygiene maintenance as it can be easy removed, repaired and surgical intervention, absence of subgingival cement. However this type of restoration requires a careful prosthetically driven implant planning, since the implant position would affect the screw access hole position. Angulated abutment can be used in divergent implants axis, when a cement-retained prosthesis is adopted. This prosthetic solution would be advisable especially when an implant is tilted too far labially and the screw access channel involves the vestibular faces or incisal edges of the restoration which can compromise the esthetics. An angulated screw channel (ASC) abutment allows to further compensate divergence up to 25 degree, and use a screw-retained restoration when a cement-retained one would have been otherwise recommended in order not to affect esthetics of the prosthetic work. At the same time, especially for posterior regions and/or in case of reduced mouth opening, this prosthetic solution would make easier and faster the tightening procedure.
Computer-guided technology improves accuracy of implant placement and minimizes anatomic limitations as well as addresses prosthetic needs with a minimally invasive approach. Moreover, divergent implants can be planned from the beginning, and the prosthodontic solutions can be simulated via virtual abutments.
The aim of this research was to investigate 3-year data from atrophic maxillary patients rehabilitated with angulated screw channel (ASC) zirconia abutments, placed on the day of surgery, to support a cemented-retained fixed dental prosthesis (FDP). This study followed the STROBE (STrengthening the Reporting of OBservational studies in Epidemiology) guidelines.
Materials and methods
This study was designed as a single cohort prospective observational study. From October 2013 to May 2014, any partial edentulous patients presenting atrophic posterior maxilla, and requiring an implant-supported FDP was considered eligible for this study. The research was performed according to the guidelines derived from the 2008 amended Helsinki Declaration. All subjects were informed about the study protocol and signed a consent form. Patients were treated in a private centre located in Rome (Italy). One clinician (MT) performed all surgical and prosthetic procedures, while two dental laboratories manufactured all the restorations.
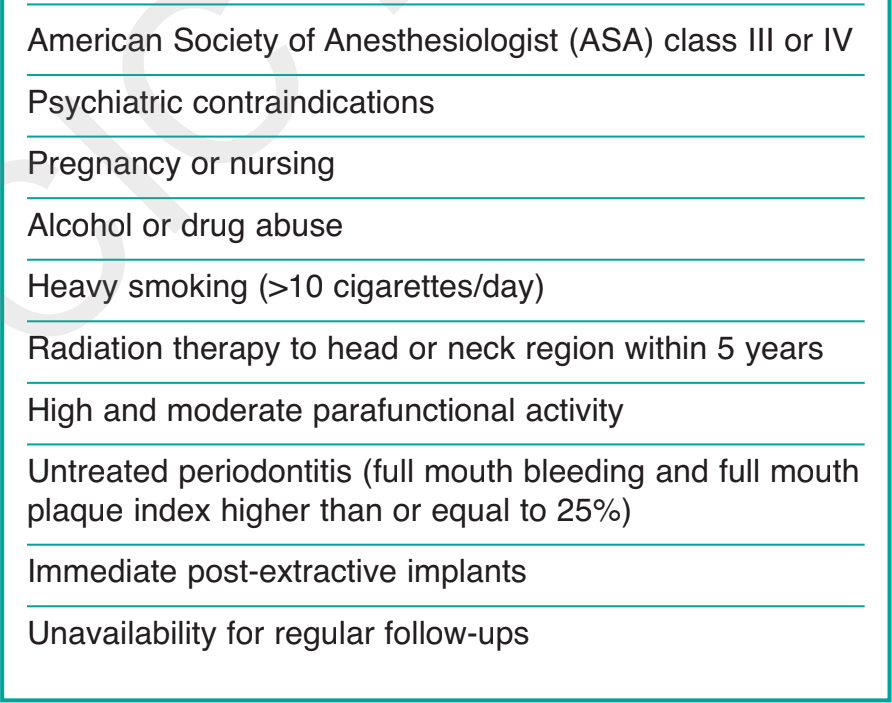
Healthy patients aged 18 years or older, who presented partial edentulism of the posterior maxilla, with Cawood-Howell Class V or VI, refused guided bone reconstruction, and able to understand and sign an informed consent form, were consecutively enrolled in this study. Hopeless teeth had to have been extracted at least 4 months before implant placement. Exclusion criteria are summarized in Table 1.
Patient medical histories, initial radiographs and models were collected for initial screening and diagnosis (Figure 1). Eligible patients received a cone beam computed tomography (CBCT) scan according to a double-scan protocol. Virtual implant planning was performed placing implants in the anterior and posterior sinus wall area, avoiding any bone reconstruction procedures.

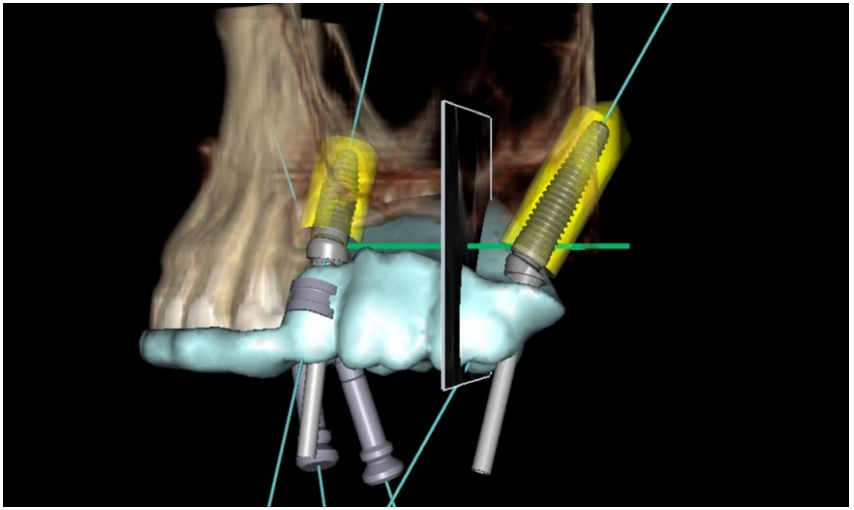
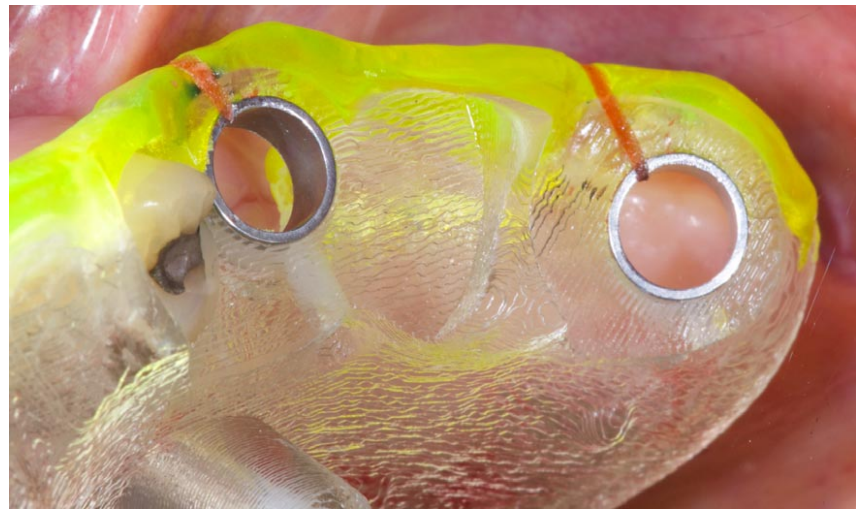
On the day of the surgery, two to three immediately loaded flapless implants (NobelReplace Conical Connection; Nobel Biocare AG, Göteborg, Sweden) were placed for each patients, using a computer-guided template assisted surgery (NobelClinician; Nobel Biocare AG). All implants were placed following a previously published protocol. Implant position and angulation were guided by the prosthetic emergence profile of the radiographic templates, derived from the diagnostic wax-up (Figure 2). Implants were placed both axially and tilted, in both the anterior and posterior sinus wall area, and in the tuberosity-pterygoid area, according to Pozzi et al. Orientation of the internal hexagon of each implant was chosen using a red line marked by the dental technician (Figure 3).
Surgical protocol
Before implant placement, surgical templates were used to fabricate master casts. Definitive white or shaded angulated screw channel (ASC) abutments were customized starting from the diagnostic wax-up, and digitalized using an optical scanner (NobelProcera, Nobel Biocare AG). All the computer aided design/computer aided manufacturing (CAD/CAM) ASC abutments were made in zirconia with a metal adaptor (Figure 4). Before surgery, each patient underwent professional oral hygiene and received specific instructions to rinse their mouth with chlorhexidine mouthwash 0.2% (1 minute, twice a day, three days prior to the surgery) (Corsodyl, Glaxo-SmithKline, Verona, Italy). Two grams of amoxicillin and clavulanic acid (Augmentin, GlaxoSmithKline, Verona, Italy) or clindamycin, 600 mg, if allergic to penicillin (Dalacin, Pfizer Sollentuna, Sweden) were administered prophylactically 1 hour prior to surgery and continued for 6 days. Local anesthesia was induced using a 4% articaine solution with epinephrine 1:100,000 (Ubistein; 3M Italy SpA, Milan, Italy). All the implants were placed flapless with the aid of a surgical template, derived from the virtual plan. Immediately after implant placement, the definitive abutments were cleaned in an ultrasonic bath with a chlorhexidine gluconate 5% solution, and then steam-cleaned for 30 seconds. Finally, the prefabricated CAD/CAM ASC abutments were screwed to the implants at 35 Ncm (Torq Control; Anthogyr, Sallanches, France). The interim acrylic restorations were cemented using a non-eugenol temporary zinc-oxide cement (TempBond NE; Kerr Dental, Switzerland) (Figure 5).


Prosthetic protocol
Three months after implant placement and loading, conventional polyvinyl siloxane impressions were taken using a 00 or 000 size retraction cord (Ultrapack; Ultradent Products Inc, South Jordan, Utah) wetted with 0.9% sodium chloride solution, for the mucosal displacement. Previously duplicated polyurethane abutments were repositioned in the definitive impression. Six months after the initial loading, definitive white or shaded CAD/CAM zirconia frameworks (NobelProcera Implant Bridge Zirconia, Nobel Biocare AG), veneered with feldspathic porcelain were cemented (Clearfil SA Cement; Kuraray Europe GmbH, Frankfurt, Germany) according to the manufacturer’s instructions and a previously published protocol (17). Before cementation, a thin layer of petroleum jelly (Vaseline; Unilever, Italy) was applied over the external marginal contour of every restoration to reduce cement adhesion over the external surface and to facilitate removal excess cement.
Occlusion and oral hygiene were carefully checked, then the patients were enrolled in an oral hygiene program and occlusion checks with recall visits every 4 months (Figure 6). Follow-up visits were scheduled annually up to 3 years after implant placement/loading (Figure 7).


Outcomes
Primary outcome measures were:
- Prosthesis failure: planned prosthesis which could not be placed, or loss of the prosthesis secondary to implant failure, or any prosthesis which had to be replaced.
- Implant failure: implants which had to be removed at implant insertion due to lack of stability, implant mobility, removal of stable implants dictated by progressive bone resorption or infection, and any complications (e.g. implant fracture) that make the implant unusable.
- Any biological or prosthetic complications.
Secondary outcome measure was:
Peri-implant marginal bone levels were evaluated on periapical radiographs taken with the paralleling technique at implant placement/loading (baseline), 1, 2 and 3 years after loading. The distance from the mesial and distal margin of the implant neck to the first bone to implant contact were measured using a dedicated software (Digora for Windows 2.8, SOREDEX, Tuusula, Finland) that was calibrated to the nearest 0.1 mm for every single image against the space between two threads, and averaged at patient level. An independent assessor (GS), not previously involved in the study, evaluated all the radiographs.
Statistical analysis
A descriptive analysis was performed for continuous data using mean±standard deviation (SD), median and 95% confidence interval (CI) (SPSS for Mac OS X version 22.0; SPSS, Chicago, IL, USA). Comparisons between each timepoint were made for each group by paired t test. All statistical comparisons were two-tailed and conducted at the 0.05 level of significance. The patient was used as the statistical unit of the analysis.
Results
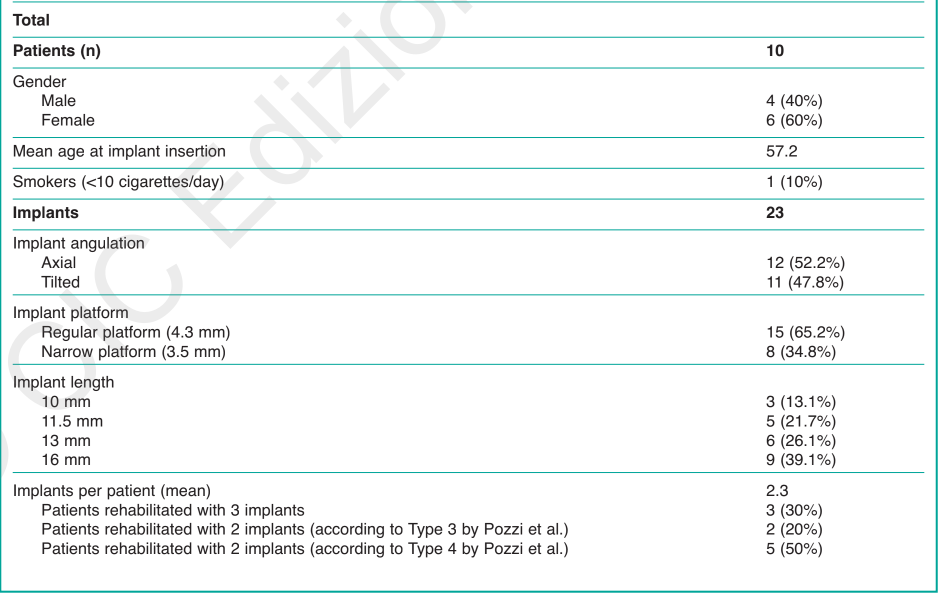
At the 3-year follow-up examination ten consecutive participants (females=6, males=4) with 23 implants 10 to 16 mm long, and the same number of angulated screw channel zirconia abutments, were consecutively included in this study. At the time of implant insertion, the patients’ age ranged from 38 to 72 years (mean age 57.2 years). Only one patient included in the study presented a slight smoking habit (< 10 cigarettes per day). Patient’s characteristics and intervention are summarized in Table 2.
During the entire follow-up period (range 36-44, mean 38.2 months), no drop-out occurred. All prostheses were stable and all implants remained osseo integrated, stable, and showed no sign of infection. Three years after loading, the implant and prosthesis cumulative survival rates were 100%. No biologic or technical complications occurred.
At baseline, the mean marginal bone level was 0.29±0.34 mm. At 1 year after implant placement and loading, the mean marginal bone level increased to 0.37±0.32 mm, and remained stable at the 2-year follow-up with the mean marginal bone level of 0.38±0.33 mm. At the last follow-up (3-year), the mean marginal bone level was 0.50±0.42 mm. During the entire follow-up period, the mean marginal bone remodeling was 0.22±0.22 mm. The main results are summarized in Table 3.
Discussions
The aim of this prospective cohort study was to investigate, over a 3-year loading period, the clinical and radiological performance of immediately loaded implants placed both axially and tilted in the posterior atrophic maxilla, and combined with angulated screw channel (ASC) zirconia abutments placed the same day of surgery. In the present study none of the implants or prosthesis failed and the 3-year after loading mean marginal bone remodeling was 0.10±0.14 mm (95% CI -0.06–0.06 mm). The major clinical conclusion of this prospective study was that the use of tilted implants in combination with ASC abutments may be considered an effective and safe alternative to maxillary sinus floor augmentation procedures when patients refuse bone reconstruction procedures. The results of the present research are slightly better than the results of a milestone manuscript published by Aparicio and colleagues in 2001. A possible explanation of this result could be that the Authors used external hexagon implants combined with conventional abutments. On the other hand, in the present study, immediately placed and loaded definitive abutments, screwed onto conical connection implants with platform switching concept were used. According to previously published randomized controlled trials, marginal bone levels were better maintained at implants restored according to the platform-switching concept. Furthermore, 3-year results of a randomized controlled trial suggest that the immediate positioning of a definitive abutment may be a possible way and strategy to minimise peri-implant crestal bone resorption of the implants. Other difference between the present investigation and the previously reported prospective study is that a different implant-abutment connection was used for the prosthetic work. Data from other two RCT suggested that internal conical connection results in lower marginal bone loss compared with the well proven external hexagon implant-abutment interface.
Pozzi et al. in 2012 published an interesting prospective study reporting data from both tilted and axial immediately loaded implants, placed using guided surgery, for the treatment of the posterior partially edentulous atrophic maxilla. Although ASC abutments were not then available, definitive CAD/CAM titanium and zirconia abutments were screwed on external hexagon implants. At the 3-year follow-up examination, the cumulative implant survival rate was 96.3%. Mean marginal bone loss from implant insertion to 3 years was 0.6±0.3 mm.
The main limitation of the present study was the small sample size that may have obscured some important information. Although no comparison was made between axial and tilted implants, Del Fabbro and Ceresoli, in a recent systematic review, found that tilting the implants does not induce significant alteration in crestal bone level change as compared to conventional axial placement after 1 year of function, even if long-term data is still scarce. These results were confirmed in a recent systematic review and meta-analysis by Monje et al. However, data from a recent prospective study found a significant correlation between implant angulation and annual bone loss for tilted implants but not for axial implants. Although a different kind of matched abutment was used (preangled or custom-angled abutment, and standard abutments), possibile explanations were that 9 out of 29 patients were bruxers and 4 out of 29 prostheses had a cantilever.
To the best of our knowledge, at the time of writing this article, there were no other published studies reporting data on immediately loaded implants placed in combination with angulated screw channel zirconia abutments. This makes it difficult to evaluate how the present results fit with other comparable studies. There is a recent cases presentation published by Gjelvold et al. This article presents three examples of single labially tilted implants restored with screw-retained single crowns cemented on customized angulated screw channel abutments used to avoid an unesthetic vestibular access channel. Nevertheless, the Authors did not draw any conclusions due to the small sample size and the very short follow-up period.
In the present study no prosthetic complications were experienced. Angulated screw channel abutments allow for angulation of the screw access channel up to 25°. These advantage enabling cement retained restoration to correct implant angulation. Computer-guided technology allows the clinician to pre-operatively plan the placement of the ASC abutment in combination with tilted implants. Divergence between implants can be measured and the prosthodontic solution can be planned according to the approved wax-up, combining the prosthetic needs with a minimally invasive approach. Furthermore, angulated screw channel abutments may also be used in case of limited interocclusal space to allow easier tightening of the abutment screw.
Finally, the presence of the metal adaptor increase the maximum join compression, avoiding risk of fracture even in case of high occlusal force, overcoming the possible mechanics drawbacks of the one-piece zirconia abutments.
Conclusions
Immediately loaded tilted and axial implants combined with ASC zirconia abutments may be considered an effective and reliable treatment option in patients refusing sinus lift surgery. Further randomized controlled trials with longer follow-up are needed.
M. Tallarico, F.M. Ceruso, E. Xhanari, M. Gargari, L. Canullo, S.M. Meloni
References
- Nevins M, Camelo M, De Paoli S, Friedland B, Schenk RK, Parma-Benfenati S, et al. A study of the fate of the buccal wall of extraction sockets of teeth with prominent roots. Int J Periodontics Restorative Dent. 2006; 26:19-29.
- Teng M, Cheng Q, Liao J, Zhang X, Mo A, Liang X. Si- nus Width Analysis and New Classification with Clinical Implications for Augmentation. Clin Implant Dent Relat Res. 2016;18:89-96.
- Esposito M, Felice P, Worthington HV. Interventions for replacing missing teeth: augmentation procedures of the maxillary sinus. Cochrane Database Syst Rev. 2014;5:CD008397.
- Aparicio C, Perales P, Rangert B. Tilted implants as an alternative to maxillary sinus grafting: a clinical, radiologic, and periotest study. Clin Implant Dent Relat Res. 2001;3:39-49.
- Del Fabbro M, Ceresoli V. The fate of marginal bone around axial vs. tilted implants: a systematic review. Eur J Oral Implantol. 2014;7:S171-89.
- Pozzi A, Sannino G, Barlattani A. Minimally invasive treatment of the atrophic posterior maxilla: A proof-of-concept prospective study with a follow-up of between 36 and 54 months. J Prosthet Dent. 2012;108:286-297.
- Barnea E, Tal H, Nissan J, Tarrasch R, Peleg M, Kolerman R. The Use of Tilted Implant for Posterior Atrophic Maxilla. Clin Implant Dent Relat Res. 2015 Apr 8. doi:10.1111/cid.12342. [Epub ahead of print]
- Chrcanovic BR, Albrektsson T, Wennerberg A. Tilted versus axially placed dental implants: A meta-analysis. J Dent. 2015;43:149-170.
- Penarrocha-Oltra D, Candel-Marti E, Ata-Ali J, Penarrocha-Diago M. Rehabilitation of the atrophic maxilla with tilted implants: review of the literature. J Oral Implantol. 2013;39:625-632.
- Monje A, Chan H-L, Suarez F, Galindo-Moreno P, Wang H-L. Marginal bone loss around tilted implants in comparison to straight implants: a meta-analysis. Int J Oral Maxillofac Implants. 2012;27:1576-1583.
- Menini M, Signori A, Tealdo T, Bevilacqua M, Pera F, Ravera G, et al. Tilted implants in the immediate loading rehabilitation of the maxilla: a systematic review. J Dent Res. 2012;91:821-827.
- Del Fabbro M, Bellini CM, Romeo D, Francetti L. Tilted implants for the rehabilitation of edentulous jaws: a systematic review. Clin Implant Dent Relat Res. 2012;14:612-621.
- Sailer I, Mühlemann S, Zwahlen M, Hämmerle CHF, Schneider D. Cemented and screw-retained implant reconstructions: a systematic review of the survival and complication rates. Clin Oral Implants Res. 2012;23:163-201.
- Pozzi A, Tallarico M, Marchetti M, Scarfo B, Esposito M. Computer-guided versus free-hand placement of immediately loaded dental implants: 1-year post-loading results of a multicentre randomised controlled trial. Eur J Oral Implantol. 2014;7:229-242.
- van Steenberghe D, Glauser R, Blomback U, Andersson M, Schutyser F, Pettersson A, et al. A computed tomographic scan-derived customized surgical template and fixed prosthesis for flapless surgery and immediate loading of implants in fully edentulous maxillae: a prospective multicenter study. Clin Implant Dent Relat Res. 2005;7:S111-120.
- Cocchetto R, Resch I, Castagna M, Vincenzi G, Celletti R. The abutment duplication technique: a novel protocol for cementable implant-supported restorations. Int J Periodontics Restorative Dent. 2010;30:415-424.
- Pozzi A, Tallarico M, Barlattani A. Monolithic lithium disilicate full-contour crowns bonded on CAD/CAM zirconia complete-arch implant bridges with 3 to 5 years of follow-up. J Oral Implantol. 2013;41:450-458.
- Canullo L, Fedele GR, Iannello G, Jepsen S. Platform switching and marginal bone-level alterations: the results of a randomized-controlled trial. Clin Oral Implants Res. 2010;21:115-121
- Pozzi A, Agliardi EL, Tallarico M, Barlattani A. Clinical and radiological outcomes of two implants with different prosthetic interfaces and neck configurations: randomized, controlled, split-mouth clinical trial. Clin Implant Dent Relat Res. 2014;16:96-106.
- Pozzi A, Tallarico M, Moy PK. Three-year post-loading results of a randomised, controlled, split-mouth trial comparing implants with different prosthetic interfaces and design in partially posterior edentulous mandibles. Eur J Oral Implantol. 2014;7:47-61.
- Canullo L, Iannello G, Götz W. The influence of individual bone patterns on peri-implant bone loss: preliminary report from a 3-year randomized clinical and histologic trial in patients treated with implants restored with matching-diameter abutments or the platform-switching concept. Int J Oral Maxillofac Implants. 2011;26:618-630.
- Canullo L, Bignozzi I, Cocchetto R, Cristalli MP, Iannello G. Immediate positioning of a definitive abutment versus repeated abutment replacements in post-extractive implants: 3-year follow-up of a randomised multicentre clinical trial. Eur J Oral Implantol. 2010;3:285-296.
- Gjelvold B, Sohrabi M, Chrcanovic B. Angled Screw Channel: An Alternative to Cemented Single-Implant Restorations - Three Clinical Examples. Int J Prosthodont. 2016;29:74-76.
- Foong JKW, Judge RB, Palamara JE, Swain MV. Fracture resistance of titanium and zirconia abutments: an in vitro study. J Prosthet Dent. 2013;109:304-312.
- Ottria L, Lauritano D, Andreasi Bassi M, Palmieri A, Candotto V, Tagliabue A, Tettamanti L. Mechanical, chemical and biological aspects of titanium and titanium alloys in implant dentistry. Journal of Biological Regulators and Homeostatic Agents. 2018;32(2):81-90.
- De Oliveira DP, Ottria L, Gargari M, Candotto V, Silvestre FJ, Lauritano D. Surface modification of titanium alloys for biomedical application: From macro to nano scale. Journal of Biological Regulators and Homeostatic Agents. 2017;31(2, Supplement 1):221-232.